Unit Project
Contents
Introduction
Literature review
On release expectations
1. Email Invite
2. Survey
3. Results
4. Implications
Night shift Charge Nurse duties
Staffing binder
Transition survey email
1. Attachment
2. Transition survey
3. Results
Transition meetings
Final preparation day
Transition day
Expansion day
Introduction
I created the task force to manage the expansion of the Pulmonary Unit from 18 beds to the evolution of 36 beds. This process began in February and continued through July of 2013. A systematic approach was adopted to identify potential problems that may occur with the expansion. An open forum of discussion was utilized to provide numerous opportunities for the thoughts and suggestions of all staff members to be heard. Surveys were distributed to all members of the Pulmonary Unit to identify concerns, rumors, and potential problems. Numerous meetings with staff members took place to discuss survey results, concerns, rumors, problems, and formulate solutions. The Pulmonary Unit's website was updated with the most recent information as it became available. The ultimate goal was to create personal ownership of this expansion for every member of the Pulmonary Unit.
Literature review
Heslop, L. & Plummer, V. (2012). Nurse staff allocation by nurse patient ratio vs a computerized nurse dependency management system: A comparative cost analysis of Australian and New Zealand hospitals. Nursing Economic$. 30 (6): 347-355. (LOE V)
Kalisch, B. & Lee, K. (2013). Variations of nursing teamwork by hospital, patient unit, and staff characteristics. Applied Nursing Research. 26 (1): 2-9. (LOE VI)
Kalisch, B, Russell, K., & Lee, K. (2013). Nursing teamwork and unit size. Western Journal of Nursing Research. 35 (2): 214-225. (LOE VI)
Nayback-Beebe, A., Forsythe, T., Funari, T., Mayfield, M., & Thomas, W. (2013). Using evidence-based leadership initiatives to create a healthy nursing work environment. Dimensions of Critical Care Nursing. 32(4): 166-173. (LOE V)
On release expectations
The first concern that occurred was on call staff members being called in early in the shift with the standard expectation that they would accept all the patient admissions. This had become more of an issue with the holidays and the unit increasing the amount of staff to prepare for the expansion. One staff member asked why the nurse being called in had to accept all the admissions and wondered why couldn't some nurses give up a patient, so that this nurse would only accept one or two patient admissions. More and more nurse were placed on call due to the Pulmonary Unit hiring more staff members in preparation for the expansion, so this problem would be occurring with increased frequency. I prepared a staff survey to determine which manner the Pulmonary Unit would treat these unique situations. Below is the actual email invite, the survey, and the results of the survey. Please note that the University of Colorado Hospital (UCH) refers to being placed "on call" as "being released."
1. Email Invite
Contents
Introduction
Literature review
On release expectations
1. Email Invite
2. Survey
3. Results
4. Implications
Night shift Charge Nurse duties
Staffing binder
Transition survey email
1. Attachment
2. Transition survey
3. Results
Transition meetings
Final preparation day
Transition day
Expansion day
Introduction
I created the task force to manage the expansion of the Pulmonary Unit from 18 beds to the evolution of 36 beds. This process began in February and continued through July of 2013. A systematic approach was adopted to identify potential problems that may occur with the expansion. An open forum of discussion was utilized to provide numerous opportunities for the thoughts and suggestions of all staff members to be heard. Surveys were distributed to all members of the Pulmonary Unit to identify concerns, rumors, and potential problems. Numerous meetings with staff members took place to discuss survey results, concerns, rumors, problems, and formulate solutions. The Pulmonary Unit's website was updated with the most recent information as it became available. The ultimate goal was to create personal ownership of this expansion for every member of the Pulmonary Unit.
Literature review
Heslop, L. & Plummer, V. (2012). Nurse staff allocation by nurse patient ratio vs a computerized nurse dependency management system: A comparative cost analysis of Australian and New Zealand hospitals. Nursing Economic$. 30 (6): 347-355. (LOE V)
Kalisch, B. & Lee, K. (2013). Variations of nursing teamwork by hospital, patient unit, and staff characteristics. Applied Nursing Research. 26 (1): 2-9. (LOE VI)
Kalisch, B, Russell, K., & Lee, K. (2013). Nursing teamwork and unit size. Western Journal of Nursing Research. 35 (2): 214-225. (LOE VI)
Nayback-Beebe, A., Forsythe, T., Funari, T., Mayfield, M., & Thomas, W. (2013). Using evidence-based leadership initiatives to create a healthy nursing work environment. Dimensions of Critical Care Nursing. 32(4): 166-173. (LOE V)
On release expectations
The first concern that occurred was on call staff members being called in early in the shift with the standard expectation that they would accept all the patient admissions. This had become more of an issue with the holidays and the unit increasing the amount of staff to prepare for the expansion. One staff member asked why the nurse being called in had to accept all the admissions and wondered why couldn't some nurses give up a patient, so that this nurse would only accept one or two patient admissions. More and more nurse were placed on call due to the Pulmonary Unit hiring more staff members in preparation for the expansion, so this problem would be occurring with increased frequency. I prepared a staff survey to determine which manner the Pulmonary Unit would treat these unique situations. Below is the actual email invite, the survey, and the results of the survey. Please note that the University of Colorado Hospital (UCH) refers to being placed "on call" as "being released."
1. Email Invite
2. Survey
3. Results
Unfortunately, the print is rather small and difficult to read. The documents were enlarged as much as the website programming would allow. Below is the reprinted version of the above four pages.
1. Email invite
Please note that the email is presented utilizing the SBAR communication tool. SBAR stands for situation, background, assessment, and recommendation. This is the hospital's preferred mode of communication. The Registered Nurse is abbreviated as RN.
From: Schadler, James C
To: UCH-Pumonary Nurses
Subject: Release RN issue
Greetings Colleagues,
S: The decreased census of the holidays resulted in nurses being placed on release and sometimes being called in to work the remainder of the shift.
B: There are two schools of thought on creating the assignment for the released nurse that is called in to work the remainder of the shift:
1. The nurse takes all the admissions and the rest of the nurses maintain their current patient assignments. Based on the timing of admissions, the supporting staff will assist with the admissions by taking report, performing the admission assessment, implementing admission orders, and ect., then providing report to hand over the patient to the nurse that was called in to work the remainder of the shift.
2. Each of the nurses give one of their patients to the nurse that was called in, resulting in all nurses being able to accept an admission. The charge nurse and the remainder of the staff will assist with admissions as needed.
A: Should the nurse on release that is called in take all the admissions or should each nurse give a patient to the nurse that is called in to work the remainder of the shift?
R: Please answer this quick 4 question survey to determine Pulmonary's best course of action on this matter.
http://www.surveymonkey.com/s/NXBFTKC
James Schadler, RN, BSN, BA
9W Pulmonary Charge Nurse
Relief Hospital Manager
University of Colorado Hospital
[email protected]
Mail Box F786
2. Survey
1. What shift do you normally work?
__Days
__Nights
2. The nurse on release is called in early to work the remainder of the shift should (8-10 hours remaining in the shift)
__take all the admission
__receive one patient from each nurse, therefore each nurse has the potential to accept an admission
3. The nurse on release is called in early to work the remainder of the shift should (4-6 hours remaining in the shift)
__take all the admissions
__receive one patient from each nurse, therefore each nurse has the potential to accept an admission
4. Do you have any thoughts or suggestions on this topic? Would the current acuity of the patients on the unit be a factor?
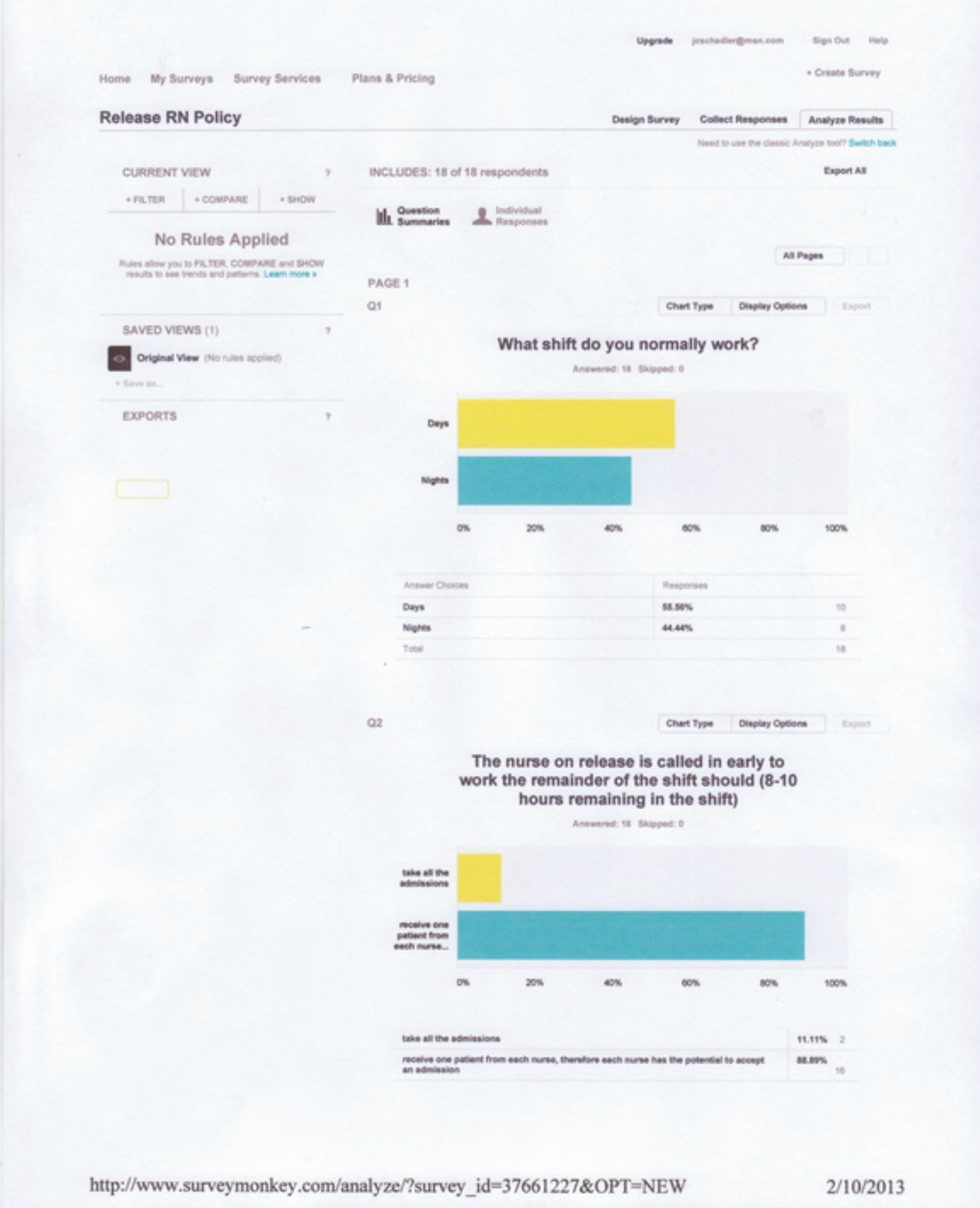
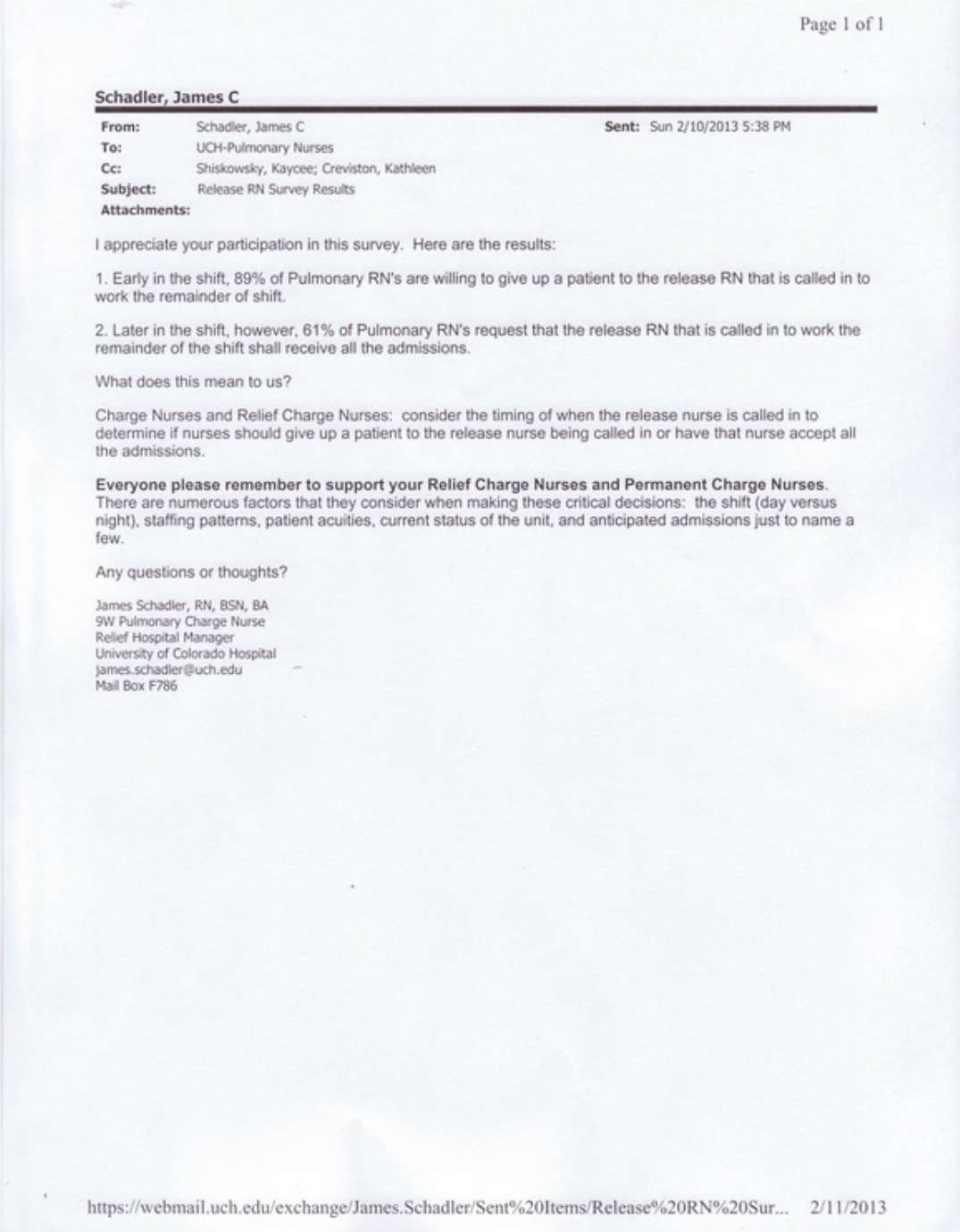
3. Results
1. 55% of the survey respondents work on the day shift and 44% of the survey respondents work on the night shift.
2. 11% of the survey respondents thought the release nurse that is called in to work the beginning of the shift should take all the admission and 89% thought the release nurse should receive one patient from each nurse, therefore each nurse has the potential to accept an admission.
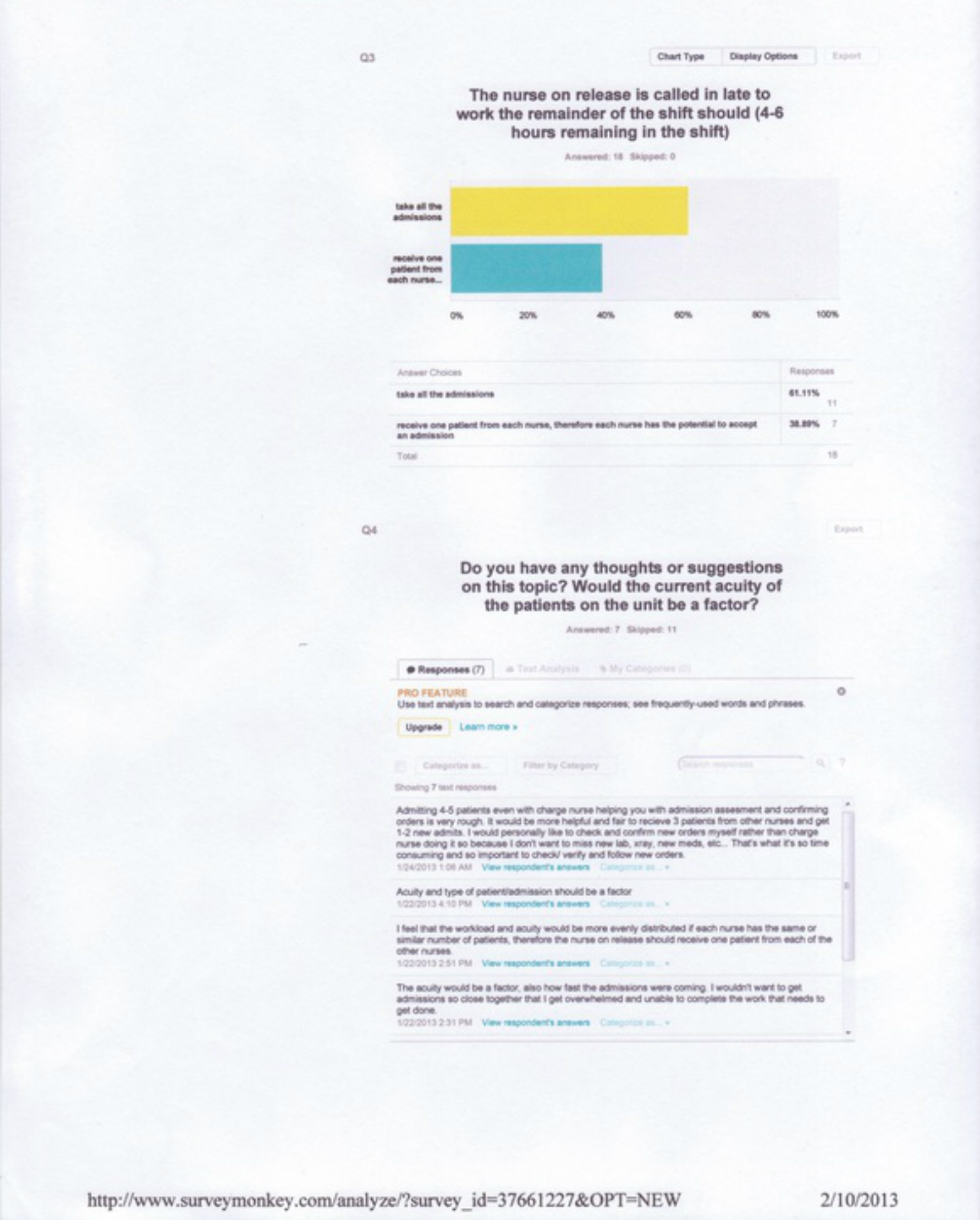
3. 61% of the survey respondents thought the release nurse that is called in to work towards the end of the shift should take all the admissions and 38% thought the release nurse should not take all the admissions.
4. The thoughts and suggestions consisted of placing heavy emphasis on the acuity level of the admissions and the timing of the admissions. One respondent even discussed the importance of acknowledging and carrying out the admission orders on their own.
4. Implications
The survey results made it obvious that the release nurse that is called in the beginning of the shift would accept patients from some of the nurses and would only accept one or two admissions. The release nurse that is called in to work in the middle of the shift would accept all the admissions. There was no significant results between the between the day and night shifts.
The results of the survey dictated how the policy would change on the Pulmonary Unit. An email was sent to all the Pulmonary Unit nurses that explained the results of the survey and how the changes to the policy would be adapted. The actual email is shown below. The permanent and relief Charge Nurses were educated on these changes during their monthly meetings. The Pulmonary Unit workflow documents were updated with these changes.
1. Email invite
Please note that the email is presented utilizing the SBAR communication tool. SBAR stands for situation, background, assessment, and recommendation. This is the hospital's preferred mode of communication. The Registered Nurse is abbreviated as RN.
From: Schadler, James C
To: UCH-Pumonary Nurses
Subject: Release RN issue
Greetings Colleagues,
S: The decreased census of the holidays resulted in nurses being placed on release and sometimes being called in to work the remainder of the shift.
B: There are two schools of thought on creating the assignment for the released nurse that is called in to work the remainder of the shift:
1. The nurse takes all the admissions and the rest of the nurses maintain their current patient assignments. Based on the timing of admissions, the supporting staff will assist with the admissions by taking report, performing the admission assessment, implementing admission orders, and ect., then providing report to hand over the patient to the nurse that was called in to work the remainder of the shift.
2. Each of the nurses give one of their patients to the nurse that was called in, resulting in all nurses being able to accept an admission. The charge nurse and the remainder of the staff will assist with admissions as needed.
A: Should the nurse on release that is called in take all the admissions or should each nurse give a patient to the nurse that is called in to work the remainder of the shift?
R: Please answer this quick 4 question survey to determine Pulmonary's best course of action on this matter.
http://www.surveymonkey.com/s/NXBFTKC
James Schadler, RN, BSN, BA
9W Pulmonary Charge Nurse
Relief Hospital Manager
University of Colorado Hospital
[email protected]
Mail Box F786
2. Survey
1. What shift do you normally work?
__Days
__Nights
2. The nurse on release is called in early to work the remainder of the shift should (8-10 hours remaining in the shift)
__take all the admission
__receive one patient from each nurse, therefore each nurse has the potential to accept an admission
3. The nurse on release is called in early to work the remainder of the shift should (4-6 hours remaining in the shift)
__take all the admissions
__receive one patient from each nurse, therefore each nurse has the potential to accept an admission
4. Do you have any thoughts or suggestions on this topic? Would the current acuity of the patients on the unit be a factor?
3. Results
1. 55% of the survey respondents work on the day shift and 44% of the survey respondents work on the night shift.
2. 11% of the survey respondents thought the release nurse that is called in to work the beginning of the shift should take all the admission and 89% thought the release nurse should receive one patient from each nurse, therefore each nurse has the potential to accept an admission.
3. 61% of the survey respondents thought the release nurse that is called in to work towards the end of the shift should take all the admissions and 38% thought the release nurse should not take all the admissions.
4. The thoughts and suggestions consisted of placing heavy emphasis on the acuity level of the admissions and the timing of the admissions. One respondent even discussed the importance of acknowledging and carrying out the admission orders on their own.
4. Implications
The survey results made it obvious that the release nurse that is called in the beginning of the shift would accept patients from some of the nurses and would only accept one or two admissions. The release nurse that is called in to work in the middle of the shift would accept all the admissions. There was no significant results between the between the day and night shifts.
The results of the survey dictated how the policy would change on the Pulmonary Unit. An email was sent to all the Pulmonary Unit nurses that explained the results of the survey and how the changes to the policy would be adapted. The actual email is shown below. The permanent and relief Charge Nurses were educated on these changes during their monthly meetings. The Pulmonary Unit workflow documents were updated with these changes.
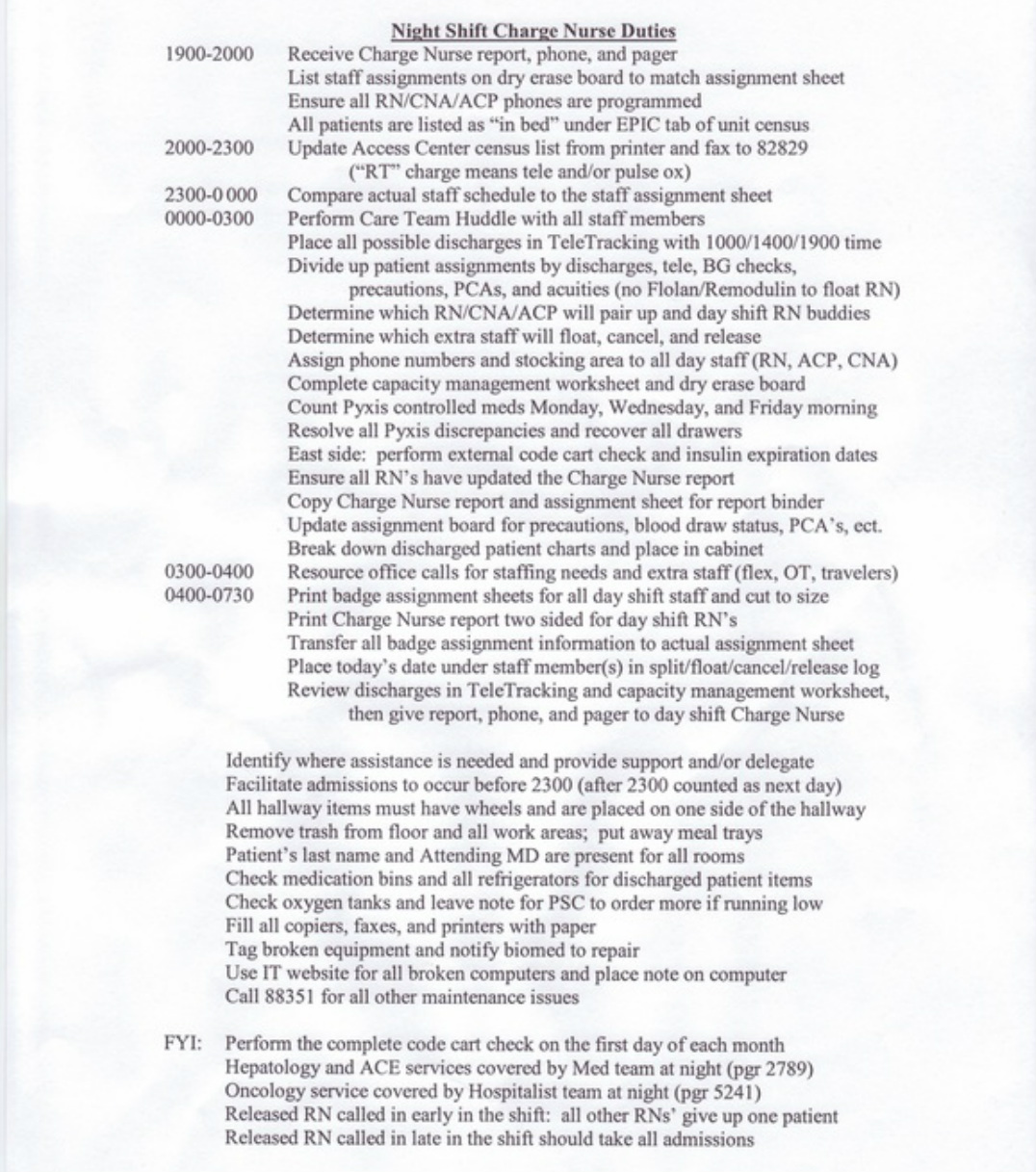
Night shift Charge Nurse duties
I created the Night Shift Charge Nurse Duties document to provide guidance for the relief Charge Nurses that do not perform that role on a consistent basis. The night shift is my normal shift of operation. These duties are updated by myself as changes occur on the unit and is stored electronically on the Pulmonary Unit's share drive. The document is also easily located in the Charge Nurse Reference binder that is near the Charge Nurse desk. The Day Shift Charge Nurse Duties document was merely updated with the release policy change as a result of the survey and is not included here since I did not create the entire document.
I created the Night Shift Charge Nurse Duties document to provide guidance for the relief Charge Nurses that do not perform that role on a consistent basis. The night shift is my normal shift of operation. These duties are updated by myself as changes occur on the unit and is stored electronically on the Pulmonary Unit's share drive. The document is also easily located in the Charge Nurse Reference binder that is near the Charge Nurse desk. The Day Shift Charge Nurse Duties document was merely updated with the release policy change as a result of the survey and is not included here since I did not create the entire document.
Staffing binder
A binder was created for documenting staffing patterns. The binder would track when staff would float, release, cancel, and be a sitter for a patient. This is essential for everyone to take their turn performing those staffing expectations. The Pulmonary Unit had shared a staffing binder with the General Surgery Unit before they moved, thus necessitating the need for a new binder and the creation of all new documents as part of the Pulmonary Unit transition process. Below is a picture of the binder..
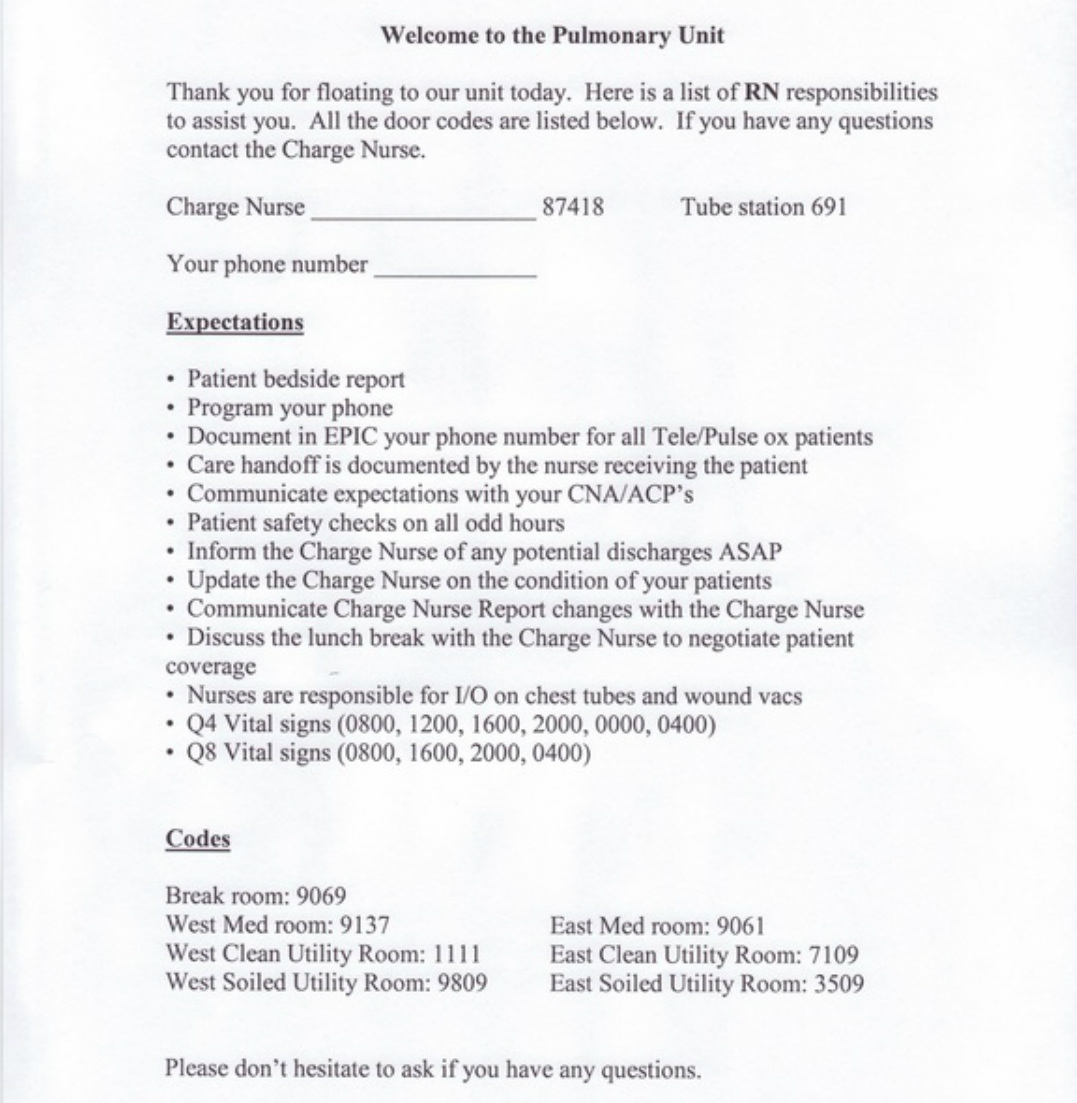
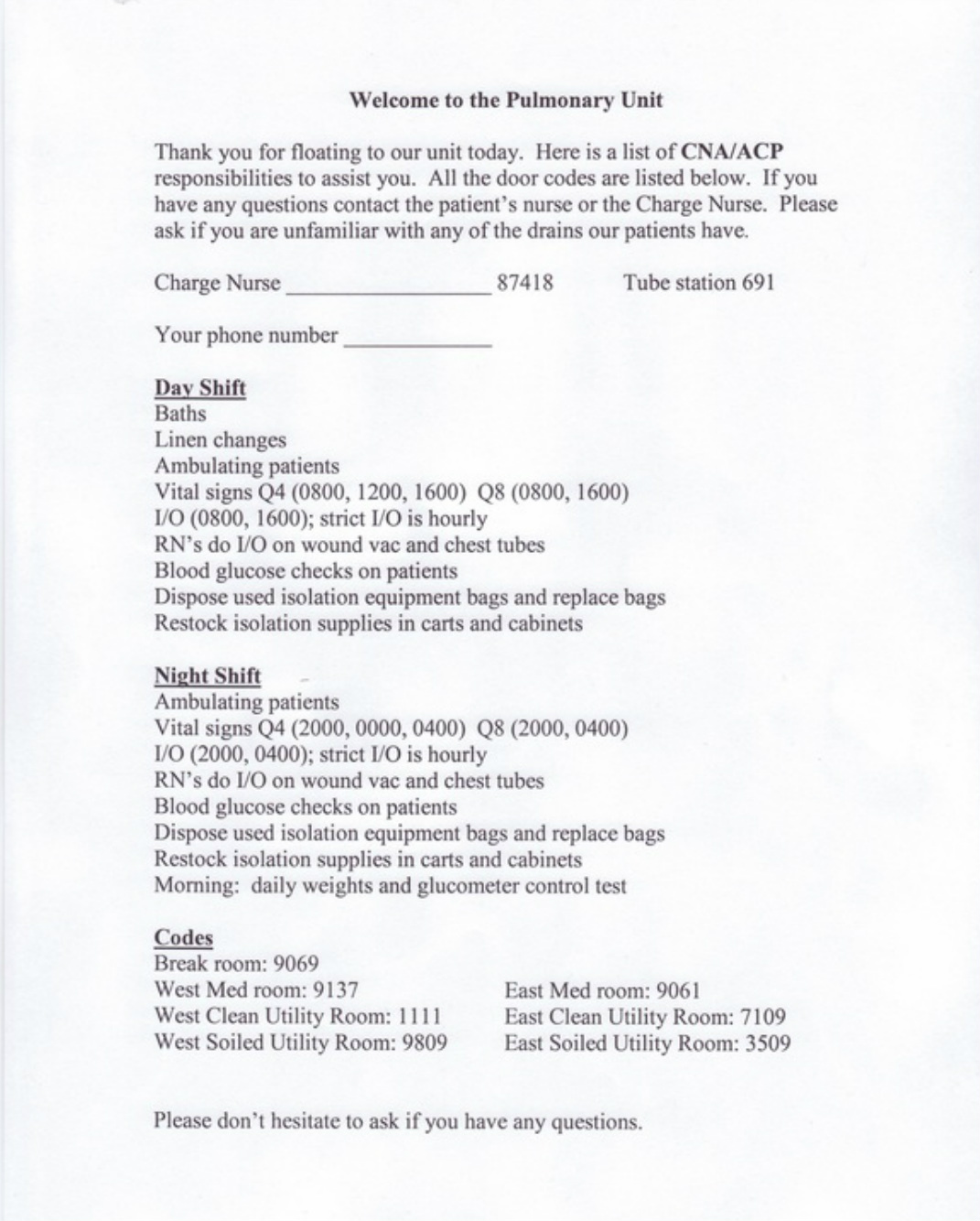
I created all the documents that are housed in this binder and will continue to update all the documents as changes occur on the Pulmonary Unit. The first document is a guide for nurses to utilize when they float to our unit and is located in a folder that is on the inside of the front cover of the binder. This form highlights the Pulmonary Units workflows, phone numbers, door codes, timing of tasks, and expectations.
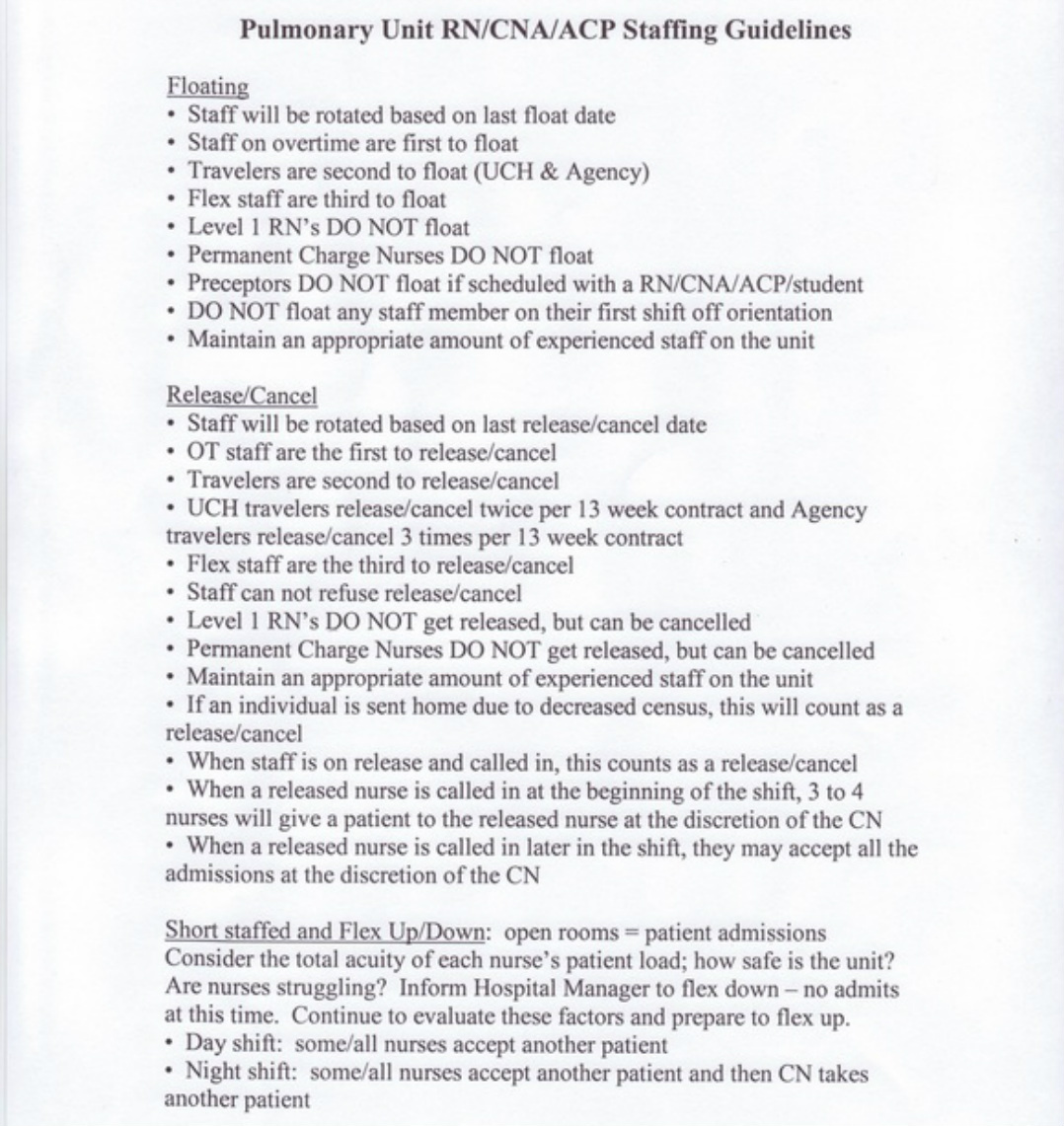
The next document in the binder is the Pulmonary Unit RN/CNA/ACP Staffing Guidelines. This is a quick reference for all staff members and a guideline for Charge Nurses to follow. The Certified Nurse Assistant is abbreviated as CNA and the Advanced Care Partner is abbreviated as ACP. They both perform the same duties but the ACP role is enhanced by expanding their responsibilities to perform some nursing duties, for they are currently enrolled in a nursing school. The staffing guidelines are shown below.
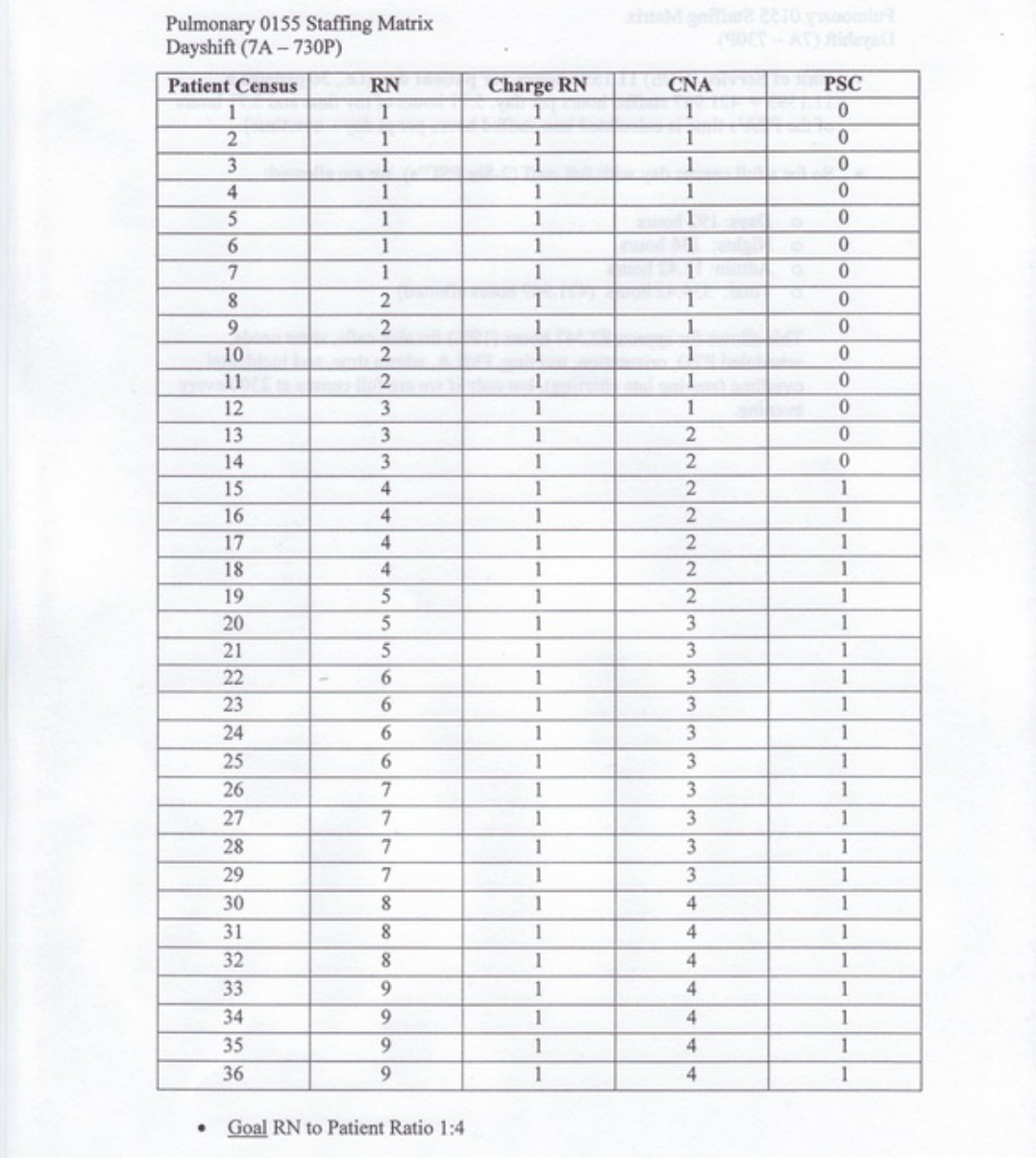
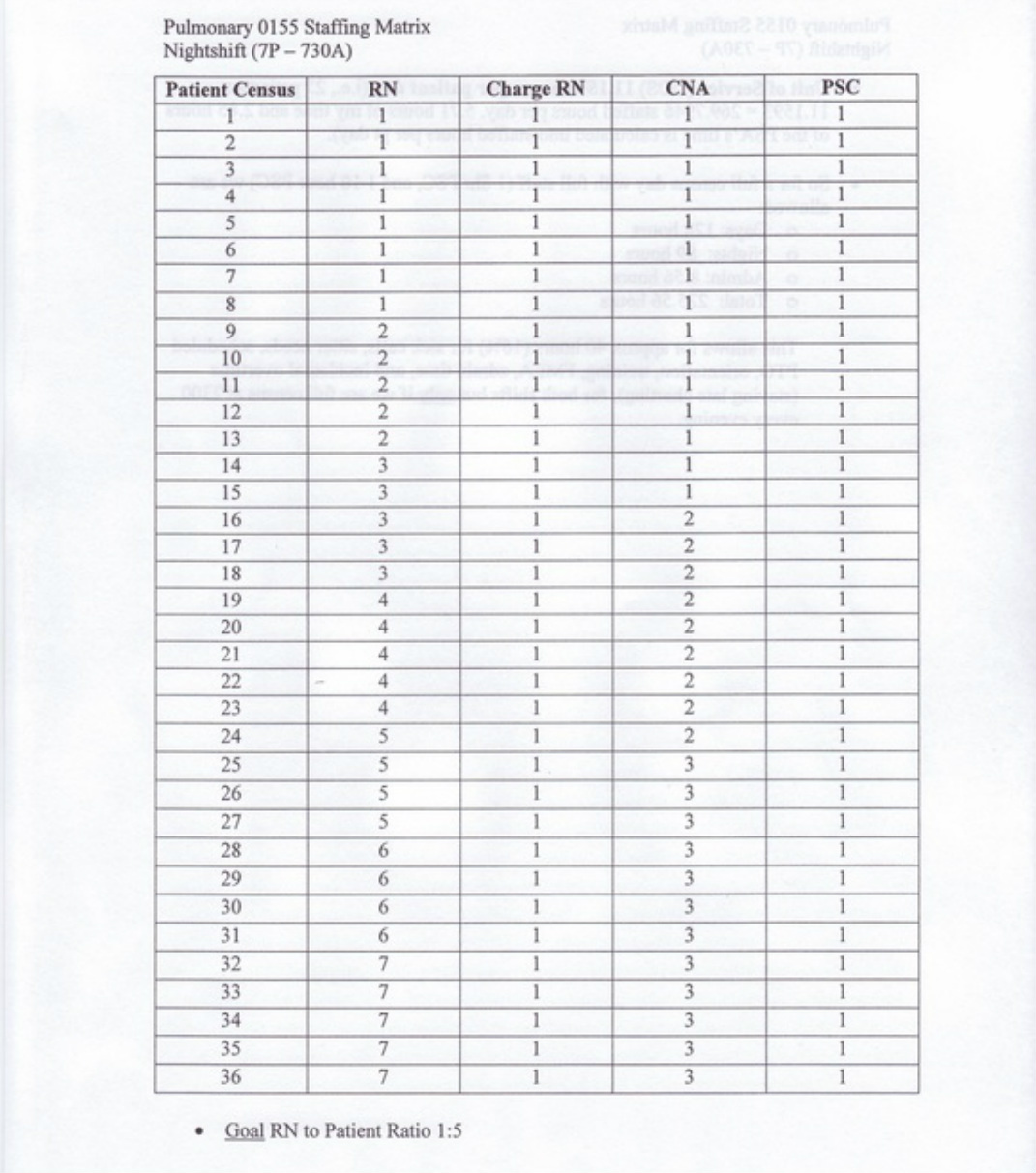
The next form in the binder is the staffing matrix. This document is a quick reference for the Charge Nurse to determine how many staff members are needed based on the current patient census. The actual matrix numbers are derived from the Pulmonary Unit's budget that allows a unit of service of 11.1593 hours per patient day. For example, the unit has 36 patients multiplied by 11.1593 to equal 401.73 staffed hours per day. The staffed hours per day breaks down into 192 hours for day shift, 136 hours for night shift, 11.42 hours of administration time, and the remainder is for variables. The variables are allocated to sick calls, sitter needs, scheduled paid time off, new employee orientation, family medical leaves, administration time, and
very diminutive amounts of overtime. Too much overtime and administrative time really hurts the budget and significantly decreases the unit's productivity numbers. Located below is the staffing matrix for the day and night shifts.
very diminutive amounts of overtime. Too much overtime and administrative time really hurts the budget and significantly decreases the unit's productivity numbers. Located below is the staffing matrix for the day and night shifts.
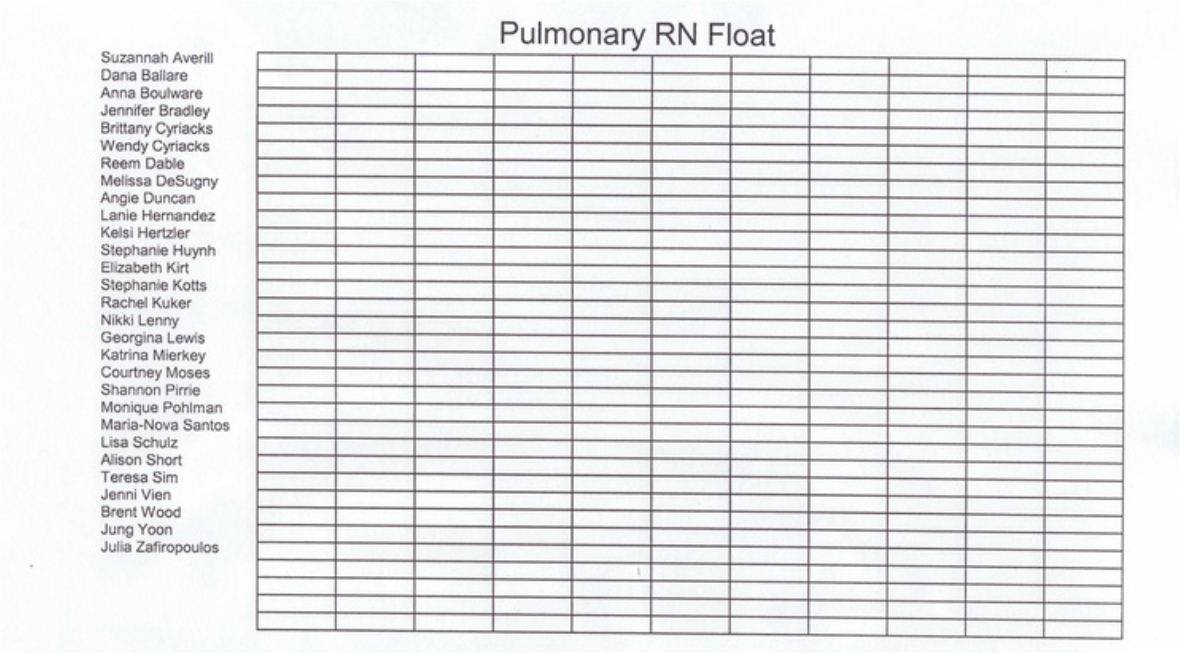
The following documents are located in the staffing binder after the staffing matrix sheets: RN float, RN cancel & release, CNA/ACP float, CNA/ACP cancel & release, and CNA/ACP sitter tracking sheets. The date is placed in the box next to the staff member's name when they float, cancel, release, or
perform the sitter function. CNA/ACP staff occasionally have to sit for a patient that is confused and unable to make rationale decisions. They maintain the safety of the patient and redirect the patient when they attempt to remove any type of medical devices that are attached to the patient.
perform the sitter function. CNA/ACP staff occasionally have to sit for a patient that is confused and unable to make rationale decisions. They maintain the safety of the patient and redirect the patient when they attempt to remove any type of medical devices that are attached to the patient.
The final item contained in the staffing binder is a form that is utilized for a CNA or ACP that floats to the Pulmonary Unit. This highlights the workflows, timing of tasks, phone numbers, door codes, and expectations. The document is located in a folder that is on the inside of the back cover of the binder.
Transition survey email
The next step was to ascertain the Pulmonary Unit's thoughts about the transition and collect suggestions that would shape the entire unit. The goal was to have everyone's input. There was already one unit that was 36 beds and we could of copied their workflows but we desired our own customized 36 bed unit to suit our particular needs and our specific patient population. Below is the email introduction of the Pulmonary Unit Transition Task Force, the attachment that details all the current information about the transition with a preview of survey questions, and the actual two page survey that was sent to all the members of the Pulmonary Unit. The detailed results of the survey follow.
1. Attachment
FYI - The Pulmonary Unit expansion will take place early this summer by
initially expanding to a 24 bed Pulmonary Unit. We will eventually expand to a 36 bed unit. At this time, there are no plans to restrict any requested time off this summer. There are some discussions taking place to convert several rooms into negative airflow rooms. The plan is to staff 4 CNA/ACP’s during the day and 3 at night when we fully expand to 36 patients. The patient to
staff ratios will not change. There are discussions taking place to have all 36 patients’ medications in both Pyxis machines and supplies for all 36 patients in each medication room. This would require the “Tap” board to be expanded to 36 patients. We are looking into the cost of these endeavors that would essentially end the need for “split” staff members. This is all the information that we have at this time. Future information will be shared by email and placed on the Pulmonary Unit's website as it comes available.
Please read each question and think of your answers in terms of specific details, please do not reply with simple “yes/no” answers. Remember, we are creating our own distinct 36 bed Pulmonary Unit.
The actual survey will be emailed to you next week.
1. What is your vision for a 36 bed Pulmonary Unit?
2. What is your perception of working a shift that would cover the entire
9th floor?
3. What would “a day in the life” look like on a 36 bed Pulmonary Unit?
4. What do you like about the Pulmonary Unit? What works well?
5. What do you dislike about the Pulmonary Unit? Do you have proposed changes?
6. What are your top 3 concerns about the expansion?
7. Please share any rumors about the expansion that you have heard.
8. One charge nurse at night for the entire floor. What is your vision for their role? What should their expectations be?
9. Two charge nurses for the day shift with the potential shift times of 6am-630pm and 8am-830pm. What is your vision for their roles? What should
their expectations be?
10. What are your thoughts about having an extra capacity nurse to assist with admissions, discharges, high acuity patients, and help out as needed?
11. We have numerous offices on the 9th floor. What are potential uses for some of these rooms?
12. There will be at least one Respiratory Therapist assigned solely to our unit. Should their role and expectations be expanded? List your thoughts
and suggestions.
13. How can we improve the process of minimizing the lost charges of supplies obtained from two medication rooms if you have patients on the east side and the west side of the 9th floor?
14. How can we improve the medication administration workflow using two different Pyxis machines if you have patients on the west side and east side of the 9th floor?
15. We may implement a tracking sheet for staff members that have patients on the west side and east side of the 9th floor, similar to what is in place now. How can we revise this mechanism?
16. Is there a patient population that you prefer? Cystic Fibrosis (CF), Pulmonary Hypertension (Phtn), Pulmonary Transplant (Ptx), or Cardiothoracic Surgery (CTS)?
17. What are the best methods to increase our staff numbers and minimize growing pains?
18. What additional aspects of training should be implemented for our new staff members?
19. The patient assignments may have one staff member (RN, CNA, ACP) with patients on the east side and west side of the 9th floor. This would involve utilizing separate medication rooms for supplies and medications. How can we improve this system?
20. The day shift would have 9 nurses taking patients and 2 charge nurses. Should charge nurses take patients on weekends? How can we boost this entire practice?
21. The night shift would have 7 nurses taking patients and a charge nurse taking 1 patient – maybe 2 patients if there are several high acuity patients. How can we enhance this process?
22. What questions do you have about the Pulmonary Unit expansion?
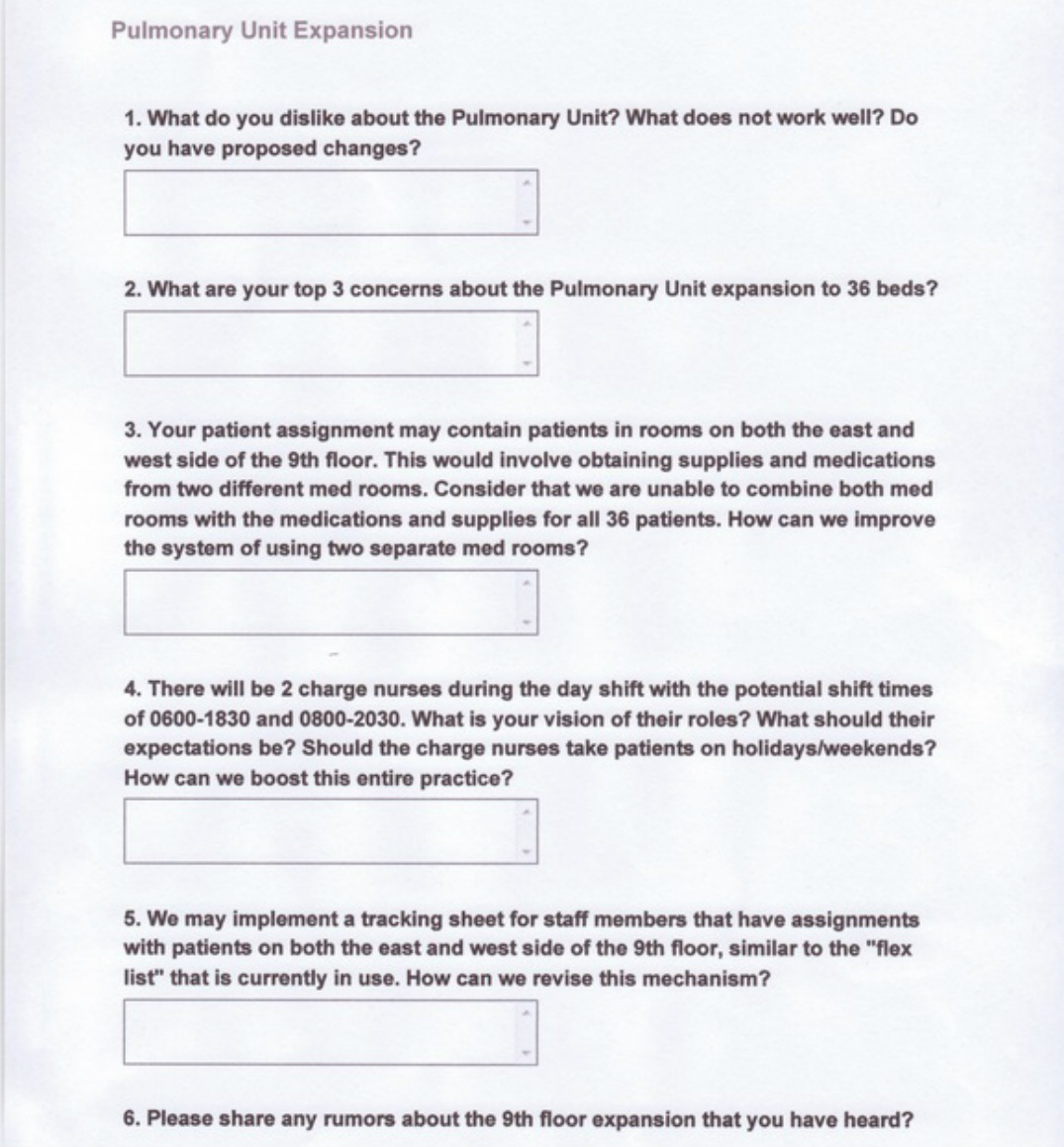
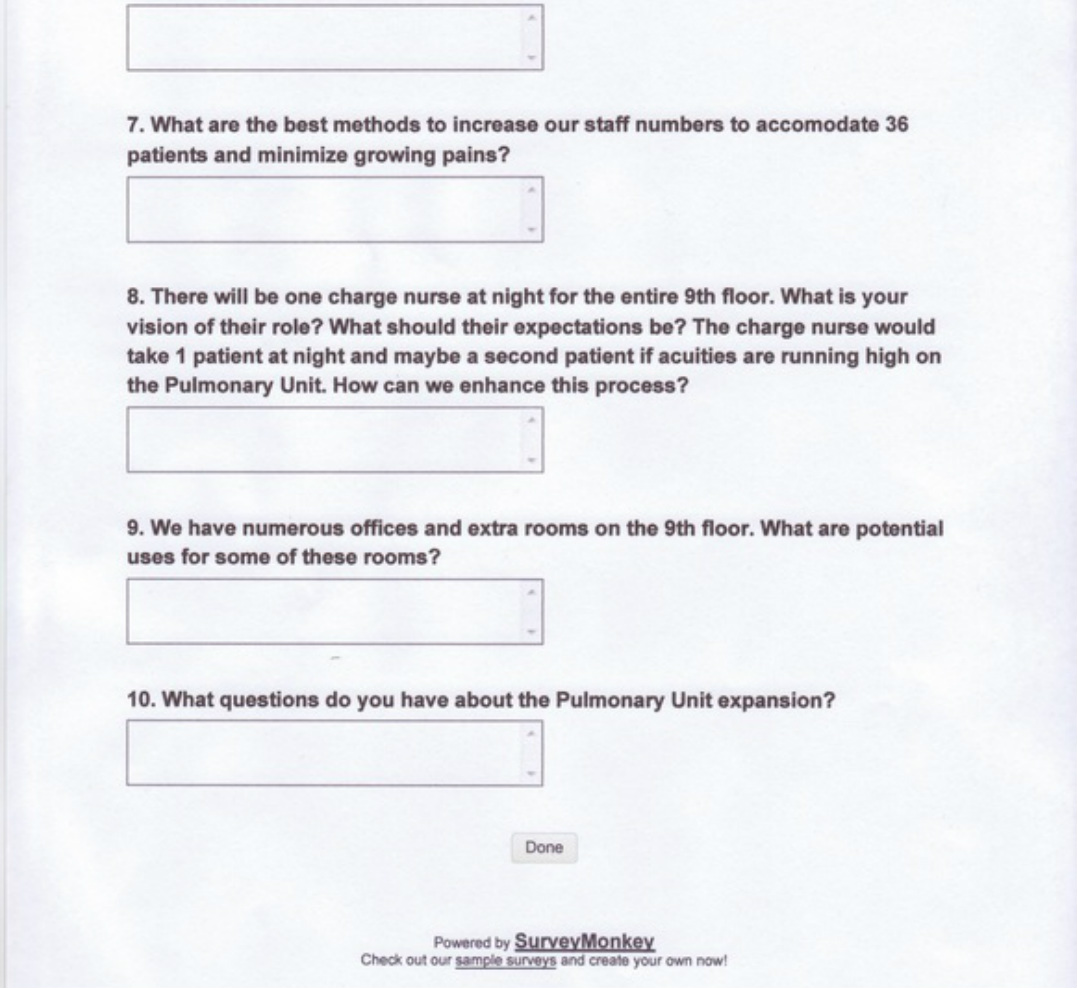
2. Transition survey
FYI - The Pulmonary Unit expansion will take place early this summer by
initially expanding to a 24 bed Pulmonary Unit. We will eventually expand to a 36 bed unit. At this time, there are no plans to restrict any requested time off this summer. There are some discussions taking place to convert several rooms into negative airflow rooms. The plan is to staff 4 CNA/ACP’s during the day and 3 at night when we fully expand to 36 patients. The patient to
staff ratios will not change. There are discussions taking place to have all 36 patients’ medications in both Pyxis machines and supplies for all 36 patients in each medication room. This would require the “Tap” board to be expanded to 36 patients. We are looking into the cost of these endeavors that would essentially end the need for “split” staff members. This is all the information that we have at this time. Future information will be shared by email and placed on the Pulmonary Unit's website as it comes available.
Please read each question and think of your answers in terms of specific details, please do not reply with simple “yes/no” answers. Remember, we are creating our own distinct 36 bed Pulmonary Unit.
The actual survey will be emailed to you next week.
1. What is your vision for a 36 bed Pulmonary Unit?
2. What is your perception of working a shift that would cover the entire
9th floor?
3. What would “a day in the life” look like on a 36 bed Pulmonary Unit?
4. What do you like about the Pulmonary Unit? What works well?
5. What do you dislike about the Pulmonary Unit? Do you have proposed changes?
6. What are your top 3 concerns about the expansion?
7. Please share any rumors about the expansion that you have heard.
8. One charge nurse at night for the entire floor. What is your vision for their role? What should their expectations be?
9. Two charge nurses for the day shift with the potential shift times of 6am-630pm and 8am-830pm. What is your vision for their roles? What should
their expectations be?
10. What are your thoughts about having an extra capacity nurse to assist with admissions, discharges, high acuity patients, and help out as needed?
11. We have numerous offices on the 9th floor. What are potential uses for some of these rooms?
12. There will be at least one Respiratory Therapist assigned solely to our unit. Should their role and expectations be expanded? List your thoughts
and suggestions.
13. How can we improve the process of minimizing the lost charges of supplies obtained from two medication rooms if you have patients on the east side and the west side of the 9th floor?
14. How can we improve the medication administration workflow using two different Pyxis machines if you have patients on the west side and east side of the 9th floor?
15. We may implement a tracking sheet for staff members that have patients on the west side and east side of the 9th floor, similar to what is in place now. How can we revise this mechanism?
16. Is there a patient population that you prefer? Cystic Fibrosis (CF), Pulmonary Hypertension (Phtn), Pulmonary Transplant (Ptx), or Cardiothoracic Surgery (CTS)?
17. What are the best methods to increase our staff numbers and minimize growing pains?
18. What additional aspects of training should be implemented for our new staff members?
19. The patient assignments may have one staff member (RN, CNA, ACP) with patients on the east side and west side of the 9th floor. This would involve utilizing separate medication rooms for supplies and medications. How can we improve this system?
20. The day shift would have 9 nurses taking patients and 2 charge nurses. Should charge nurses take patients on weekends? How can we boost this entire practice?
21. The night shift would have 7 nurses taking patients and a charge nurse taking 1 patient – maybe 2 patients if there are several high acuity patients. How can we enhance this process?
22. What questions do you have about the Pulmonary Unit expansion?
2. Transition survey
3. Results
1. What do you dislike about the Pulmonary Unit? What does not work well? Do you have proposed changes?
Centralized Ansos sheets.
Overflow of med/surg pts.
Propose change-prioritize our pt population for admit.
Revamp care team station: centralized assignment board for all 36 patients.
Move shared equipment (tele monitor, fax, ect.) to central location.
New grads take too long to level up. Don’t delay so long making new RN’s
relief Charge Nurse (CN).
Have all supplies in one central location.
Staff bathroom; more bathrooms in general.
Acuity chart to determine how many ACP/CNA’s are needed.
4 ACP/CNA’s at night if floor has many high acuity patients.
0600 blood draws done on time, not at 0730.
Compensate RN’s when taking on larger pt assignment when a RN is pulled
from our unit.
New hires work nights only for the first year. This should be an expectation.
Concerned that 36 bed unit will have trouble staffing RN’s to work night shift.
Flow is good, no immediate changes.
Better coordination between RN’s and Pulmonary teams.
Same issues keep occurring with CF, CTS, & other Plm patients, that never get resolved.
Suggest committee where common issues are discussed and solutions
provided to MD services (drug seeking, dependency issues with CF
population)
Clean utility room too far down the hall (brown and red socks in
different places)
Best practices/expectations for new residents/fellows.
All bathing items should be stored together.
CNA/ACP’s should devise how/where items are stored.
Better organization of supplies, stocking of some items seem arbitrary.
Lack of communication between MD’s and RN’s
Need to know MD goals of patients/nurses to facilitate timely discharges.
Suggest MD’s communicate to Charge Nurse about patient goals/discharge
date/time.
I don’t like the attitude of staff towards conflicts with pts. When you have a problem with a patient you have to remember that they may be in a state
where they can’t function as a perfect person.
For all staff to continue educating the pt on the importance of calling RN directly.
Answering call lights for beeping pumps.
None.
2. What are your top 3 concerns about the Pulmonary Unit expansion to 36
beds?
Experienced nurses to staff unit. Mostly junior or inexperienced staff.
Off service patients and increased patient loads.
Unit cohesion and organization.
Not having experienced nurses on the floor; hire only new grads.
Having to take more than 4 patients (more than 5 at night).
Not having enough staff for a doubling in size.
Having enough experienced nurses to staff entire floor.
Having a lot of medicine overflow patients.
Staffing (experienced RN’s).
Getting dumped on by ED/medicine patients when we aren’t full with Pulm
patients.
Not having 1500 tea time when General Surgery moves.
Understaffing, caring for too many patients.
Charge Nurse, split nurse, and supply room.
Staffing issues: will there be more instances for RN’s released or cancelled?
Will there be uneven patient assignments if the unit is not full?
Will we be fully staffed before expanding to 36 beds (RN, CNA, Perm CN)?
Staffing, pyxis (another would be nice), leadership (more perm CN).
How many nurses on during day shift? Night shift?
Having enough staff, especially CNA/ACP’s during shifts.
Equipment in good working condition.
Communication about changes.
Time to restock hall closets with what we use in pulmonary.
Time to respond to bed alarms, ect., when pts on 9W & 9E.
None.
3. Your patient assignment may contain patients in rooms on both the east and west side of the 9th floor. This would involve obtaining supplies and medications from two different med rooms. Consider that we are unable to combine both med rooms with the medications and supplies for all 36 patients. How can we improve the system of using two separate med
rooms?
Do our best to keep assignments to one med room, when possible.
Keep the patients closer to the Care Team Station to at least cut down
on the distance.
Could we tap out for PAR excellence for all 36 patients on either side?
Stock 2nd supply room with pertinent supplies (Flolan tubing, pleurevac containers).
One person split per shift (like we are doing now), minimize staff that has to split.
Being able to tap out for both sides in the same med room.
Pyxis machines that accommodate all 36 patients in both med rooms.
Two pt scan boards and all meds in both Pyxis machines.
Patient placement is very important when split.
All pt meds stocked in appropriate side of the floor.
Do not make nurses run east end to west end: group split assignment close.
By making sure we tap all supplies on the right side of the unit.
Employee education on utilizing the “borrow” tap.
Communicate with CNA/ACP as soon as pt is assigned to the floor: earlier
time to get supplies together.
Keep CF pts on 9W and all other pts on 9E: specialize what is stocked on both sides.
Making sure we tap supplies and communicate with RN’s about use of supplies.
Charge Nurse make sure doctors tap, even if they have to watch them a couple of times.
4. There will be 2 Charge Nurses during the day shift with potential shift
times of 0600-1830 and 0800-2030. What is your vision of their roles? Should Charge Nurses take patients on holidays/weekends? How can we
boost this entire practice?
CN work together to manage all 36 beds and one goes to bed control meeting.
Each manage 18 beds, but have each other as a resource to the entire floor.
Schedule 1 perm CN & 1 relief CN but keep the times the same.
One CN should round with CF/CTS/Pulm Htn teams.
CN should be able to take patients if necessary.
CN take patients on weekends/holidays.
During the week CN should not take patients and be an experienced resource.
CN assist staff with busy patient loads and settle in new admits.
CN assist with all IV meds requiring a cosign.
CN be a resource with out patients on weekdays but take pts on weekend/ holidays.
2 charge nurses, really?
Perm CN early shift & relief CN take pts
Admit/discharge help, assist with busy patients.
Weekend/holidays charge nurse takes patients.
Perm CN attend capacity meetings and relief CN tend to floor needs.
CN’s buddy up with RN’s to track their needs throughout the shift.
Lots of communication between CN’s to divide tasks & ensure to update capacity issues.
5. We may implement a tracking sheet for staff members that have assignments with patients on both the east and west side of the 9th floor, similar to the “split nurse” tracking log that is currently in use. How can we revive this mechanism?
I really don’t think this is necessary, we are one floor.
Do away with it all together: assignments should consider walking distance.
I think we continue to use the split sheet as we have in the past.
Too much of an extra burden, all patients will be Pulmonary patients.
Explore work-arounds to the 2 Pyxis problem.
The system that is currently in place works just fine.
I think that all nurses should have patients on both sides.
Keep it as a rotation among all RN’s to be fair.
More effort to assign the split nurse in rooms close to the middle of the floor.
Have the Charge Nurse track important tasks that need to be done.
Try and give RN’s their pts on the same side.
6. Please share any rumors about the 9th floor expansion that you have
heard.
We will get a bunch of medicine patients.
Will I need to brush up on my CIWA skills?
We may expand to a few step-down beds.
In order to become a relief CN, you will have to be med/surg certified.
Our sister unit will be AIP2, 9th floor medicine, so we can expect more of those pts.
Heard no rumors.
Are we pairing with medicine or surgery?
Step-down beds-what does this mean in terms of nurse-patient ratios?
What additional training will we need for step-down beds?
Med-Subspecialties Unit on the 9th floor AIP2 will provide overflow patients to us.
Only 4 Permanent Charge Nurses for 36 beds?
We may have a lot of CF pts.
None, I don’t care.
None.
7. What are the best methods to increase our staff numbers to accommodate 36 patients and minimize growing pains?
Make sure a mix of experienced nurses with new staff.
Hire other experienced nurses, not all new grads.
Hire the travelers from the Med-Surg ED unit.
Most of our experienced RN’s work nights… transfer some of them to day
shift.
Hire some experienced nurses and ACP’s that have worked on our floor.
Hire some experienced nurses, as well as new grads.
Start hiring experienced nurses and continue to hire/train new grads.
Experienced nurses and new grads… not all new grads!!!
Traveler or agency RN’s to fill in before we hire them permanently.
Only open beds when you have the staff to cover them.
Hiring and being overstaffed ahead of time seems to be buffing up staff
numbers.
Throwing in a few experienced RN’s.
Recruiting for the open position that has been online for several months.
Hire and train: people are getting married and knocked up.
Hire extra people including flex and part time.
Rotating staff during weekends.
Keep staff that can consistently keep a set schedule.
We are always going to have growing pains.
8. There will be one Charge Nurse at night for the entire 9th floor. What is your vision of their role? The Charge Nurse would take 1 patient at night and maybe a second patient if acuities are running high on the Pulmonary Unit. How can we enhance this process?
Night Charge Nurse has no patients to assist with busy patients.
1 patient max. They have to be a resource for the entire floor, which will be
challenging.
Share duties with day shift Charge Nurses (2 code cart checks).
Night Charge Nurse takes the heaviest acuity patient on the unit.
Take 1 patient anywhere on the unit.
Night Charge Nurse has no patients to be a resource for the entire unit.
One low acuity patient only – be available for helping others.
Helping more with admits, late discharges, and transfers.
One easy patient so that they can cosign for all high risk medications.
One Charge Nurse for 36 patients should have no patients to be a
resource to staff.
Only 1 easy patient for Charge Nurse should be the maximum amount.
1 patient only; must be in charge of 7 RN’s and 3 CNA/ACP’s.
Only 1 easy patient; must be a resource for everyone, including Dr’s.
9. We have numerous offices and extra rooms on the 9th floor. What are potential uses for some of these rooms?
CF workout room (6 staff requested this).
Perhaps a zen lounge for quiet time for stressed staff (5 staff requests this).
Nicer family meeting room with computer(s) for them to use (4 RN requests for this).
Pumping room for all the new mamas (3 staff requests this).
A separate break room where staff can rest (3 staff requests this).
Employee bathroom with shower (3 staff requests this).
A visitor sleeping room (2 staff requests this).
Pyxis room: 3rd Pyxis would decrease waiting in line for getting meds.
RT or home O2 office.
Pharmacist office.
Outfit larger conference room with a projector and computer.
A separate staff break room with radio, TV, and sofa (no food mess present).
Patient solariums.
Employee time out, like a break room.
Entertainment for patients.
A lounge or another locker room.
One room for all the exercise bikes.
One room for VS machines.
Patient and family education room.
10. What questions do you have about the Pulmonary Unit expansion?
When are we hiring more Charge Nurses?
Do we get to keep Matt as our floor pharmacist?
Will there be more RT’s?
Will we still have a PSC during the day?
Will we have to take more than: 4 patients on day or 5 at night?
Equipment upgrades: VS machines, patient TV’s, IV poles, walkers, ect.?
Will there be a capacity nurse during the day?
Can we try to keep pt assignments on one side of the floor to avoid confusion?
How is it gonna work with SW, CM, pharmacists, and RT’s?
Can we keep our rock star Matt Casiano?
Will we be getting any new/additional equipment?
What physical changes/updates can we do to the entire 9th floor?
Fix tired old break room, cluttered care team station, tiny & sweltering solarium?
When is this gonna happen?
Will it effect the schedule?
What happens if staffing needs fall short?
None.
Transition meetings
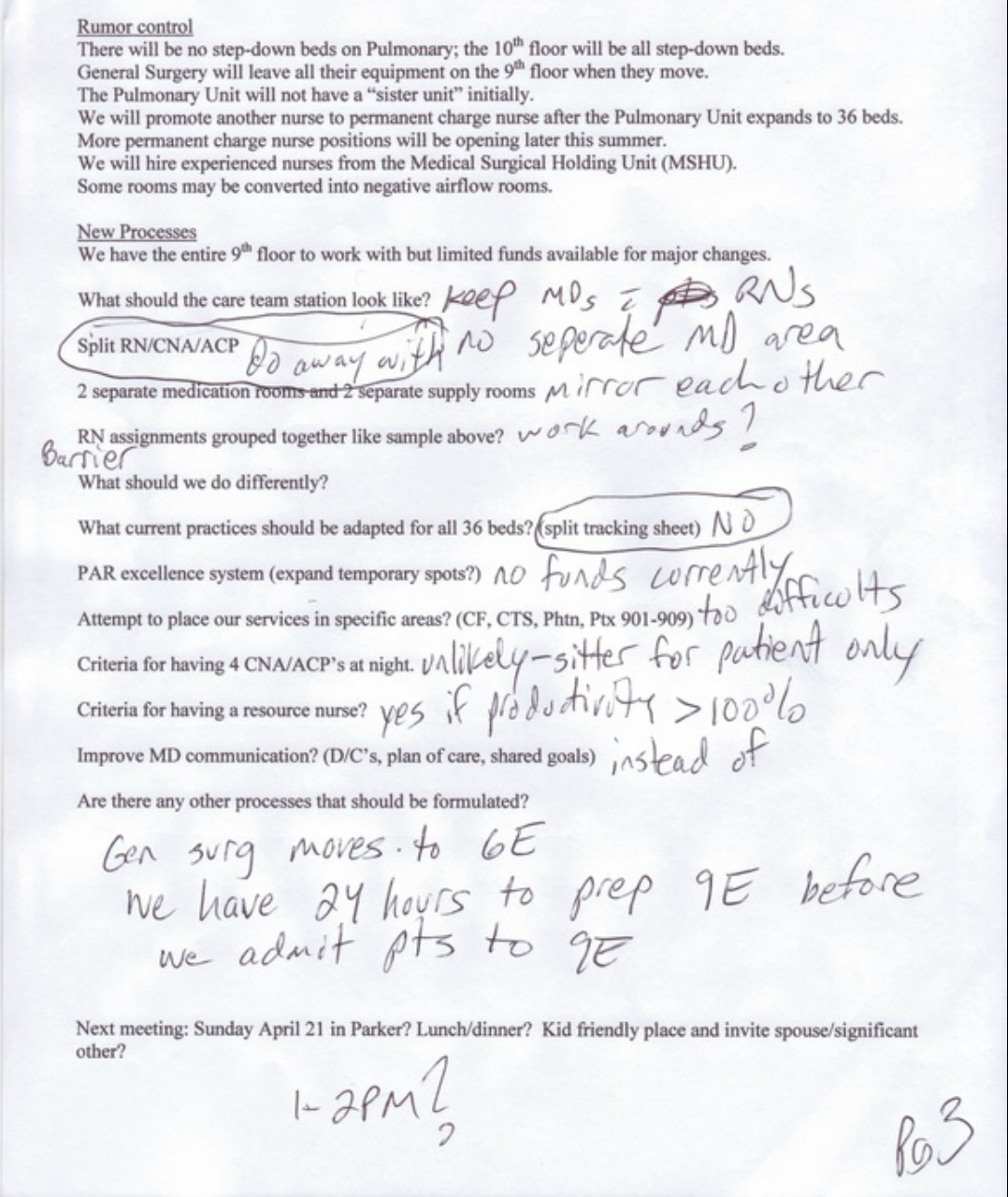
The next item on the agenda was to address the rumors and concerns that were derived from the survey. An email was sent out to the Pulmonary Unit team and the Pulmonary Unit website was updated. The following information was placed in both of those areas: there will be no step-down beds on the Pulmonary unit, another Permanent Charge Nurse will be promoted after the unit expands to 36 beds, another Permanent Charge Nurse will be promoted towards the end of the summer, the transition will take place the first week of June, and General Surgery will leave all the equipment behind when they move.
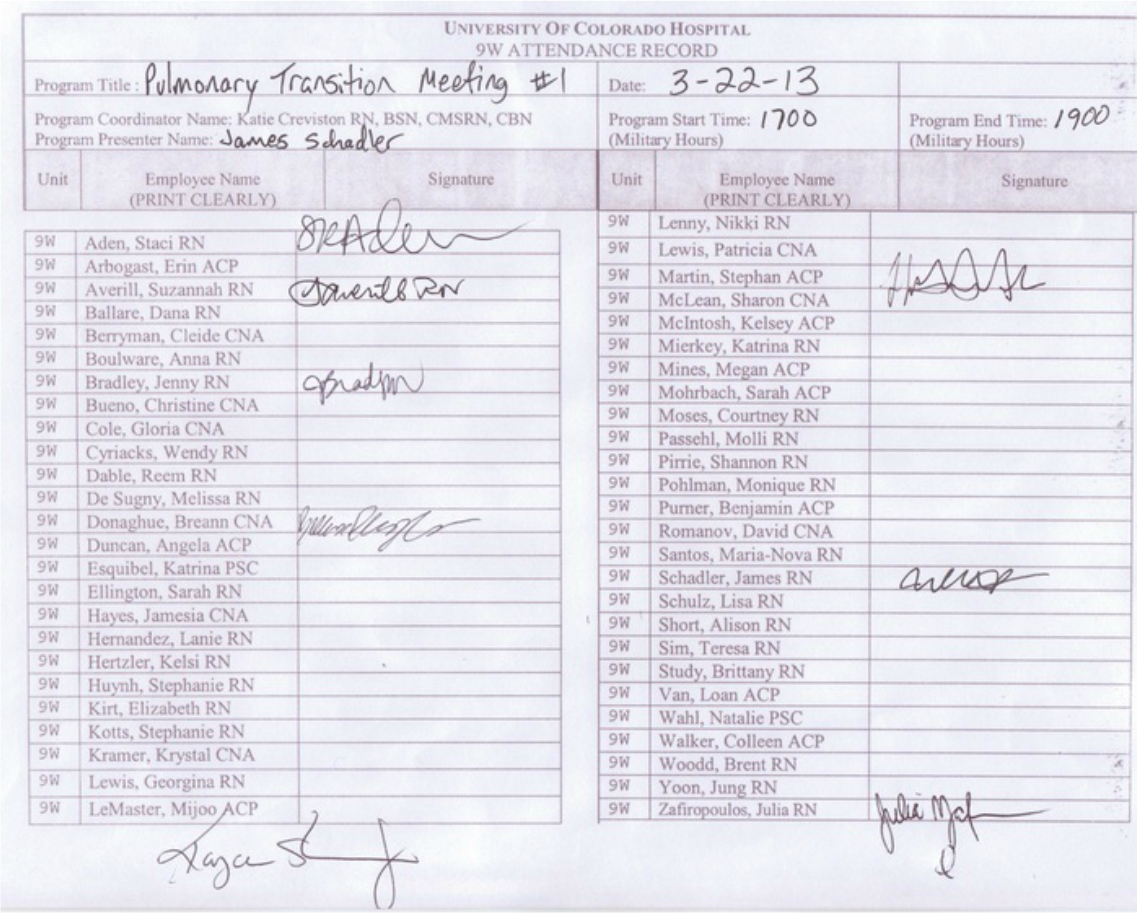
The first Pulmonary transition meeting was arranged for March 22, 2013 at a nurse's house. I thought a neutral area off campus would decrease the
anxiety generated from the hospital, lead to more open discussions, formulate outside of the box, and really allow the creative juices to flow. Each meeting was a potluck meal and staff members were encouraged to bring significant others and children. Below is the agenda for the first meeting with some notes that I took during the meeting and the attendance record. Please excuse my penmanship, for my printing is rather clear and concise but the notes were taken on clipboard while trying to maintain eye contact with the speaker.
1. What do you dislike about the Pulmonary Unit? What does not work well? Do you have proposed changes?
Centralized Ansos sheets.
Overflow of med/surg pts.
Propose change-prioritize our pt population for admit.
Revamp care team station: centralized assignment board for all 36 patients.
Move shared equipment (tele monitor, fax, ect.) to central location.
New grads take too long to level up. Don’t delay so long making new RN’s
relief Charge Nurse (CN).
Have all supplies in one central location.
Staff bathroom; more bathrooms in general.
Acuity chart to determine how many ACP/CNA’s are needed.
4 ACP/CNA’s at night if floor has many high acuity patients.
0600 blood draws done on time, not at 0730.
Compensate RN’s when taking on larger pt assignment when a RN is pulled
from our unit.
New hires work nights only for the first year. This should be an expectation.
Concerned that 36 bed unit will have trouble staffing RN’s to work night shift.
Flow is good, no immediate changes.
Better coordination between RN’s and Pulmonary teams.
Same issues keep occurring with CF, CTS, & other Plm patients, that never get resolved.
Suggest committee where common issues are discussed and solutions
provided to MD services (drug seeking, dependency issues with CF
population)
Clean utility room too far down the hall (brown and red socks in
different places)
Best practices/expectations for new residents/fellows.
All bathing items should be stored together.
CNA/ACP’s should devise how/where items are stored.
Better organization of supplies, stocking of some items seem arbitrary.
Lack of communication between MD’s and RN’s
Need to know MD goals of patients/nurses to facilitate timely discharges.
Suggest MD’s communicate to Charge Nurse about patient goals/discharge
date/time.
I don’t like the attitude of staff towards conflicts with pts. When you have a problem with a patient you have to remember that they may be in a state
where they can’t function as a perfect person.
For all staff to continue educating the pt on the importance of calling RN directly.
Answering call lights for beeping pumps.
None.
2. What are your top 3 concerns about the Pulmonary Unit expansion to 36
beds?
Experienced nurses to staff unit. Mostly junior or inexperienced staff.
Off service patients and increased patient loads.
Unit cohesion and organization.
Not having experienced nurses on the floor; hire only new grads.
Having to take more than 4 patients (more than 5 at night).
Not having enough staff for a doubling in size.
Having enough experienced nurses to staff entire floor.
Having a lot of medicine overflow patients.
Staffing (experienced RN’s).
Getting dumped on by ED/medicine patients when we aren’t full with Pulm
patients.
Not having 1500 tea time when General Surgery moves.
Understaffing, caring for too many patients.
Charge Nurse, split nurse, and supply room.
Staffing issues: will there be more instances for RN’s released or cancelled?
Will there be uneven patient assignments if the unit is not full?
Will we be fully staffed before expanding to 36 beds (RN, CNA, Perm CN)?
Staffing, pyxis (another would be nice), leadership (more perm CN).
How many nurses on during day shift? Night shift?
Having enough staff, especially CNA/ACP’s during shifts.
Equipment in good working condition.
Communication about changes.
Time to restock hall closets with what we use in pulmonary.
Time to respond to bed alarms, ect., when pts on 9W & 9E.
None.
3. Your patient assignment may contain patients in rooms on both the east and west side of the 9th floor. This would involve obtaining supplies and medications from two different med rooms. Consider that we are unable to combine both med rooms with the medications and supplies for all 36 patients. How can we improve the system of using two separate med
rooms?
Do our best to keep assignments to one med room, when possible.
Keep the patients closer to the Care Team Station to at least cut down
on the distance.
Could we tap out for PAR excellence for all 36 patients on either side?
Stock 2nd supply room with pertinent supplies (Flolan tubing, pleurevac containers).
One person split per shift (like we are doing now), minimize staff that has to split.
Being able to tap out for both sides in the same med room.
Pyxis machines that accommodate all 36 patients in both med rooms.
Two pt scan boards and all meds in both Pyxis machines.
Patient placement is very important when split.
All pt meds stocked in appropriate side of the floor.
Do not make nurses run east end to west end: group split assignment close.
By making sure we tap all supplies on the right side of the unit.
Employee education on utilizing the “borrow” tap.
Communicate with CNA/ACP as soon as pt is assigned to the floor: earlier
time to get supplies together.
Keep CF pts on 9W and all other pts on 9E: specialize what is stocked on both sides.
Making sure we tap supplies and communicate with RN’s about use of supplies.
Charge Nurse make sure doctors tap, even if they have to watch them a couple of times.
4. There will be 2 Charge Nurses during the day shift with potential shift
times of 0600-1830 and 0800-2030. What is your vision of their roles? Should Charge Nurses take patients on holidays/weekends? How can we
boost this entire practice?
CN work together to manage all 36 beds and one goes to bed control meeting.
Each manage 18 beds, but have each other as a resource to the entire floor.
Schedule 1 perm CN & 1 relief CN but keep the times the same.
One CN should round with CF/CTS/Pulm Htn teams.
CN should be able to take patients if necessary.
CN take patients on weekends/holidays.
During the week CN should not take patients and be an experienced resource.
CN assist staff with busy patient loads and settle in new admits.
CN assist with all IV meds requiring a cosign.
CN be a resource with out patients on weekdays but take pts on weekend/ holidays.
2 charge nurses, really?
Perm CN early shift & relief CN take pts
Admit/discharge help, assist with busy patients.
Weekend/holidays charge nurse takes patients.
Perm CN attend capacity meetings and relief CN tend to floor needs.
CN’s buddy up with RN’s to track their needs throughout the shift.
Lots of communication between CN’s to divide tasks & ensure to update capacity issues.
5. We may implement a tracking sheet for staff members that have assignments with patients on both the east and west side of the 9th floor, similar to the “split nurse” tracking log that is currently in use. How can we revive this mechanism?
I really don’t think this is necessary, we are one floor.
Do away with it all together: assignments should consider walking distance.
I think we continue to use the split sheet as we have in the past.
Too much of an extra burden, all patients will be Pulmonary patients.
Explore work-arounds to the 2 Pyxis problem.
The system that is currently in place works just fine.
I think that all nurses should have patients on both sides.
Keep it as a rotation among all RN’s to be fair.
More effort to assign the split nurse in rooms close to the middle of the floor.
Have the Charge Nurse track important tasks that need to be done.
Try and give RN’s their pts on the same side.
6. Please share any rumors about the 9th floor expansion that you have
heard.
We will get a bunch of medicine patients.
Will I need to brush up on my CIWA skills?
We may expand to a few step-down beds.
In order to become a relief CN, you will have to be med/surg certified.
Our sister unit will be AIP2, 9th floor medicine, so we can expect more of those pts.
Heard no rumors.
Are we pairing with medicine or surgery?
Step-down beds-what does this mean in terms of nurse-patient ratios?
What additional training will we need for step-down beds?
Med-Subspecialties Unit on the 9th floor AIP2 will provide overflow patients to us.
Only 4 Permanent Charge Nurses for 36 beds?
We may have a lot of CF pts.
None, I don’t care.
None.
7. What are the best methods to increase our staff numbers to accommodate 36 patients and minimize growing pains?
Make sure a mix of experienced nurses with new staff.
Hire other experienced nurses, not all new grads.
Hire the travelers from the Med-Surg ED unit.
Most of our experienced RN’s work nights… transfer some of them to day
shift.
Hire some experienced nurses and ACP’s that have worked on our floor.
Hire some experienced nurses, as well as new grads.
Start hiring experienced nurses and continue to hire/train new grads.
Experienced nurses and new grads… not all new grads!!!
Traveler or agency RN’s to fill in before we hire them permanently.
Only open beds when you have the staff to cover them.
Hiring and being overstaffed ahead of time seems to be buffing up staff
numbers.
Throwing in a few experienced RN’s.
Recruiting for the open position that has been online for several months.
Hire and train: people are getting married and knocked up.
Hire extra people including flex and part time.
Rotating staff during weekends.
Keep staff that can consistently keep a set schedule.
We are always going to have growing pains.
8. There will be one Charge Nurse at night for the entire 9th floor. What is your vision of their role? The Charge Nurse would take 1 patient at night and maybe a second patient if acuities are running high on the Pulmonary Unit. How can we enhance this process?
Night Charge Nurse has no patients to assist with busy patients.
1 patient max. They have to be a resource for the entire floor, which will be
challenging.
Share duties with day shift Charge Nurses (2 code cart checks).
Night Charge Nurse takes the heaviest acuity patient on the unit.
Take 1 patient anywhere on the unit.
Night Charge Nurse has no patients to be a resource for the entire unit.
One low acuity patient only – be available for helping others.
Helping more with admits, late discharges, and transfers.
One easy patient so that they can cosign for all high risk medications.
One Charge Nurse for 36 patients should have no patients to be a
resource to staff.
Only 1 easy patient for Charge Nurse should be the maximum amount.
1 patient only; must be in charge of 7 RN’s and 3 CNA/ACP’s.
Only 1 easy patient; must be a resource for everyone, including Dr’s.
9. We have numerous offices and extra rooms on the 9th floor. What are potential uses for some of these rooms?
CF workout room (6 staff requested this).
Perhaps a zen lounge for quiet time for stressed staff (5 staff requests this).
Nicer family meeting room with computer(s) for them to use (4 RN requests for this).
Pumping room for all the new mamas (3 staff requests this).
A separate break room where staff can rest (3 staff requests this).
Employee bathroom with shower (3 staff requests this).
A visitor sleeping room (2 staff requests this).
Pyxis room: 3rd Pyxis would decrease waiting in line for getting meds.
RT or home O2 office.
Pharmacist office.
Outfit larger conference room with a projector and computer.
A separate staff break room with radio, TV, and sofa (no food mess present).
Patient solariums.
Employee time out, like a break room.
Entertainment for patients.
A lounge or another locker room.
One room for all the exercise bikes.
One room for VS machines.
Patient and family education room.
10. What questions do you have about the Pulmonary Unit expansion?
When are we hiring more Charge Nurses?
Do we get to keep Matt as our floor pharmacist?
Will there be more RT’s?
Will we still have a PSC during the day?
Will we have to take more than: 4 patients on day or 5 at night?
Equipment upgrades: VS machines, patient TV’s, IV poles, walkers, ect.?
Will there be a capacity nurse during the day?
Can we try to keep pt assignments on one side of the floor to avoid confusion?
How is it gonna work with SW, CM, pharmacists, and RT’s?
Can we keep our rock star Matt Casiano?
Will we be getting any new/additional equipment?
What physical changes/updates can we do to the entire 9th floor?
Fix tired old break room, cluttered care team station, tiny & sweltering solarium?
When is this gonna happen?
Will it effect the schedule?
What happens if staffing needs fall short?
None.
Transition meetings
The next item on the agenda was to address the rumors and concerns that were derived from the survey. An email was sent out to the Pulmonary Unit team and the Pulmonary Unit website was updated. The following information was placed in both of those areas: there will be no step-down beds on the Pulmonary unit, another Permanent Charge Nurse will be promoted after the unit expands to 36 beds, another Permanent Charge Nurse will be promoted towards the end of the summer, the transition will take place the first week of June, and General Surgery will leave all the equipment behind when they move.
The first Pulmonary transition meeting was arranged for March 22, 2013 at a nurse's house. I thought a neutral area off campus would decrease the
anxiety generated from the hospital, lead to more open discussions, formulate outside of the box, and really allow the creative juices to flow. Each meeting was a potluck meal and staff members were encouraged to bring significant others and children. Below is the agenda for the first meeting with some notes that I took during the meeting and the attendance record. Please excuse my penmanship, for my printing is rather clear and concise but the notes were taken on clipboard while trying to maintain eye contact with the speaker.
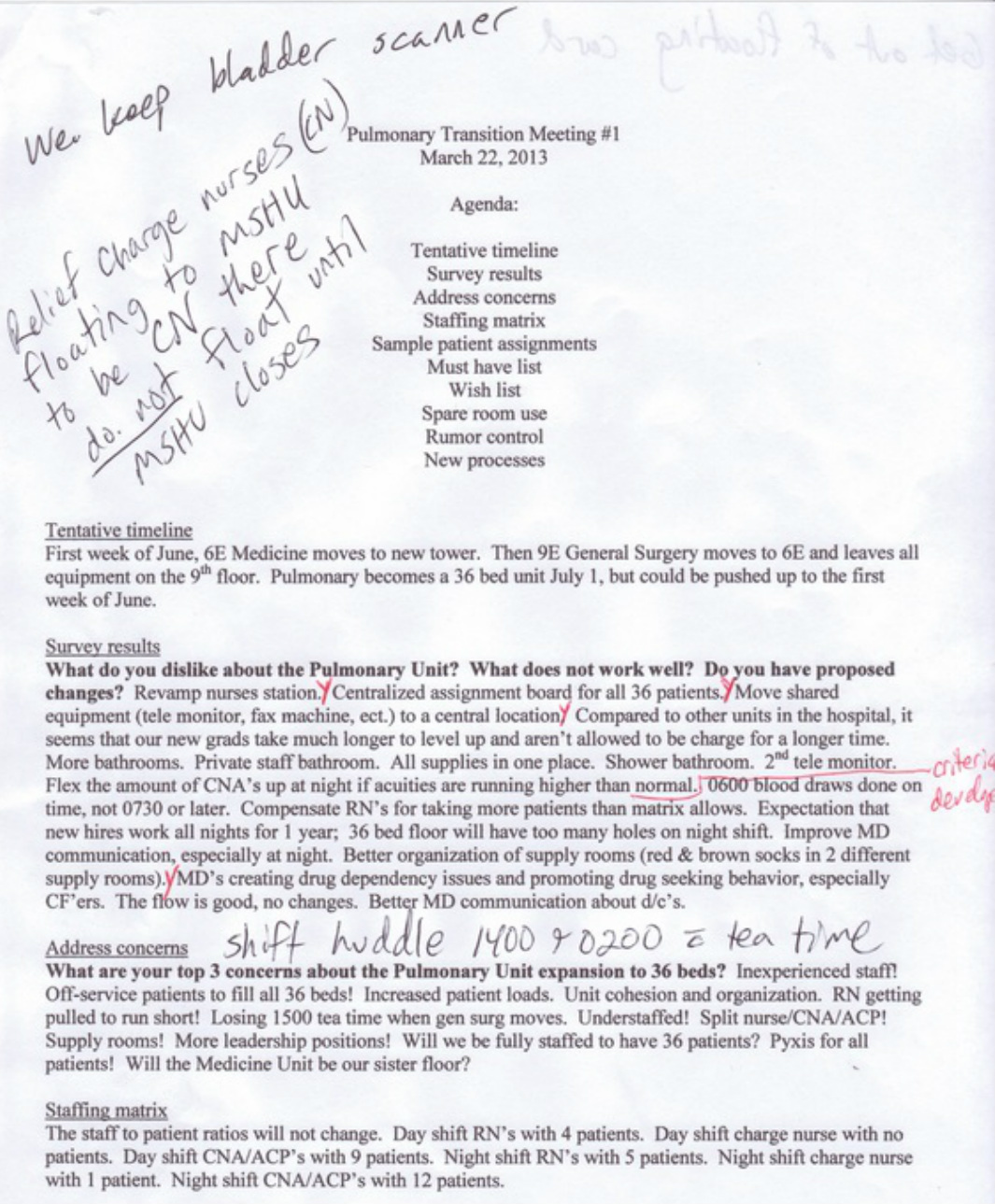
The first meeting was a great success and the Pulmonary Unit Manager, Kaycee was able to attend. Some of the survey results were discussed and a significant change was noted: we have the space but not the budget for major changes. A wish list was developed for the future and it was determined what changes would take place when the General Surgery Unit moved to the 6th floor.
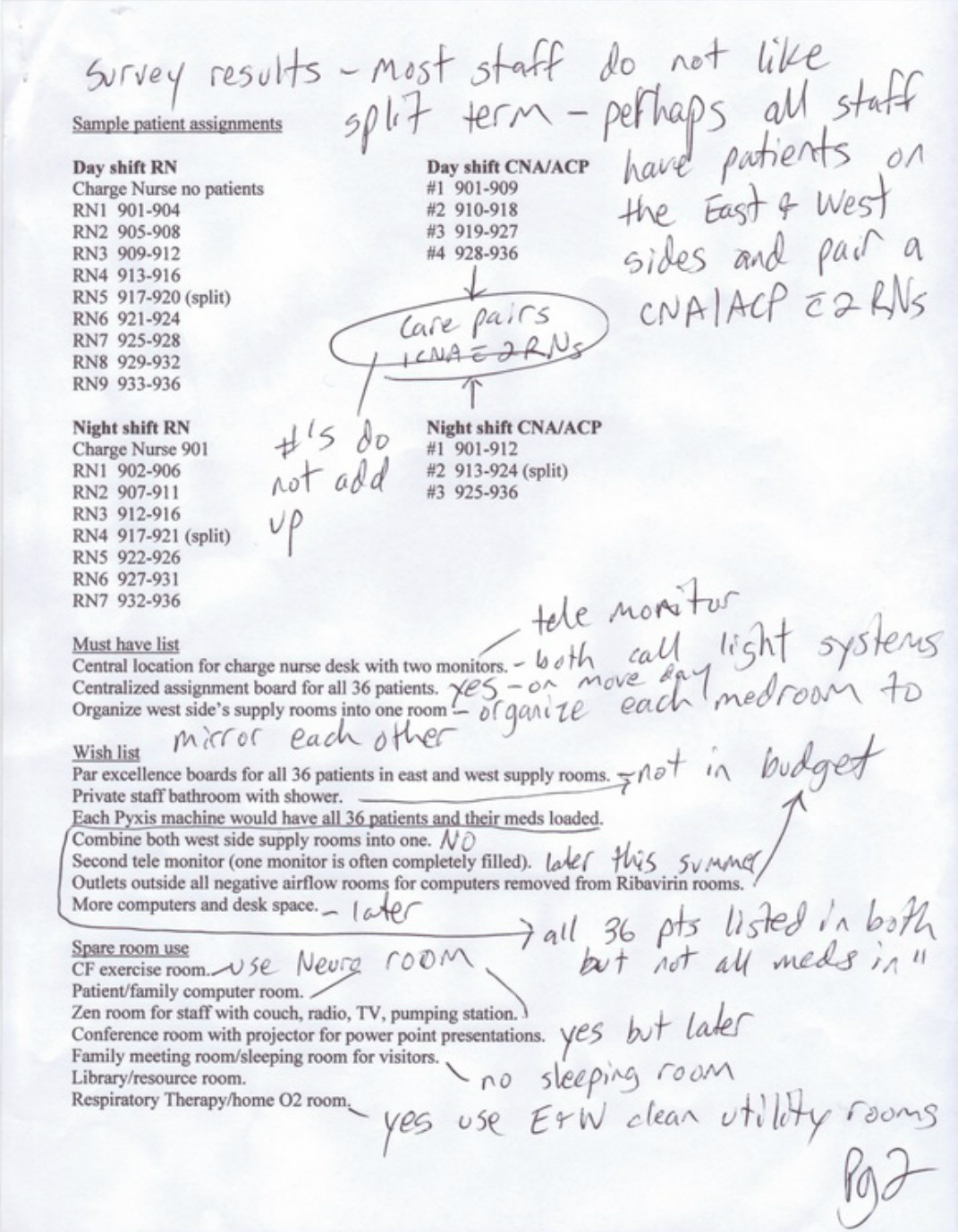
Another surprising change that came about this meeting was the thought that the term "split" would go away. This practice was utilized when we shared staff with the General Surgery Unit. I had already created forms to track which nurses and aides had split assignments so that each staff member would take turns with this endeavor. This translates to mean that all nurses and aides would have patients on both the east and west side of the 9th floor. Medications and supplies would be obtained for the patients on their corresponding sides. Rooms 901 - 918 are on the west side and rooms 919 - 936 are on the east side. For example, a patient in room 909 would require staff to retrieve supplies and medications from the west side medication/supply room and a patient in room 928 would require staff to retrieve supplies and medications from the east side medication/supply room.
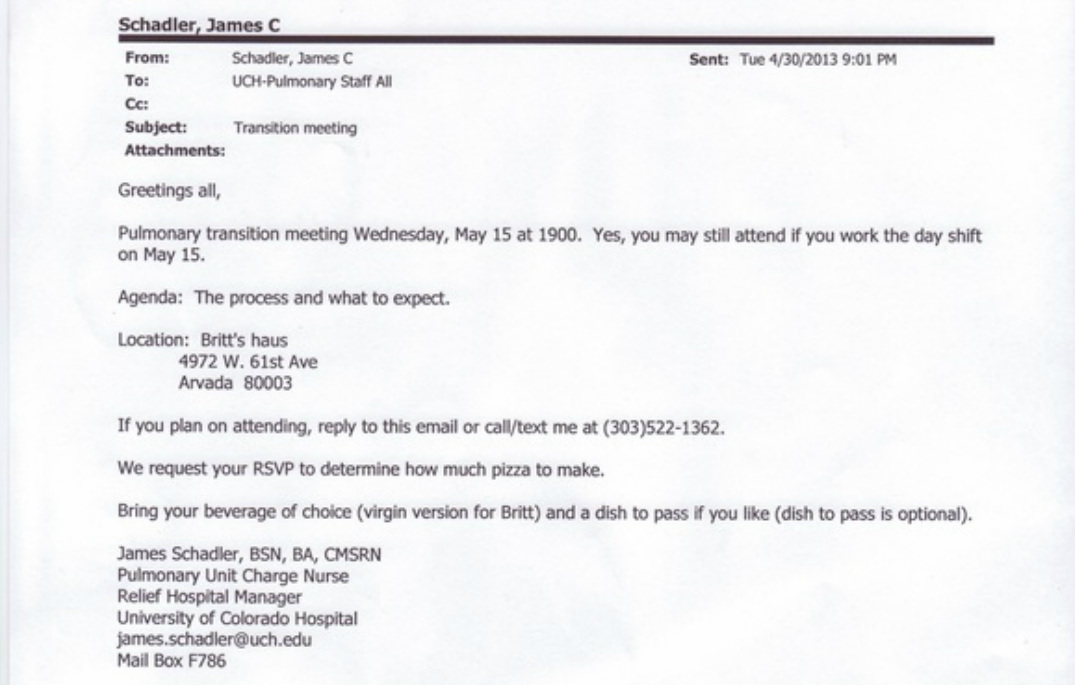
The results of the meeting were emailed to all Pulmonary Unit staff. Numerous manager, charge nurse, and staff meetings were conducted to disseminate the information. Staff input was collected utilizing individual and group conversations, email, phone calls, and text messaging. Below is the invite for the second meeting, the agenda with notes, the admission plan, and the attendance record. The meeting agenda also included the complete survey results but that document is not included here because it was placed far above this tab with the actual survey questions.
Another surprising change that came about this meeting was the thought that the term "split" would go away. This practice was utilized when we shared staff with the General Surgery Unit. I had already created forms to track which nurses and aides had split assignments so that each staff member would take turns with this endeavor. This translates to mean that all nurses and aides would have patients on both the east and west side of the 9th floor. Medications and supplies would be obtained for the patients on their corresponding sides. Rooms 901 - 918 are on the west side and rooms 919 - 936 are on the east side. For example, a patient in room 909 would require staff to retrieve supplies and medications from the west side medication/supply room and a patient in room 928 would require staff to retrieve supplies and medications from the east side medication/supply room.
The results of the meeting were emailed to all Pulmonary Unit staff. Numerous manager, charge nurse, and staff meetings were conducted to disseminate the information. Staff input was collected utilizing individual and group conversations, email, phone calls, and text messaging. Below is the invite for the second meeting, the agenda with notes, the admission plan, and the attendance record. The meeting agenda also included the complete survey results but that document is not included here because it was placed far above this tab with the actual survey questions.
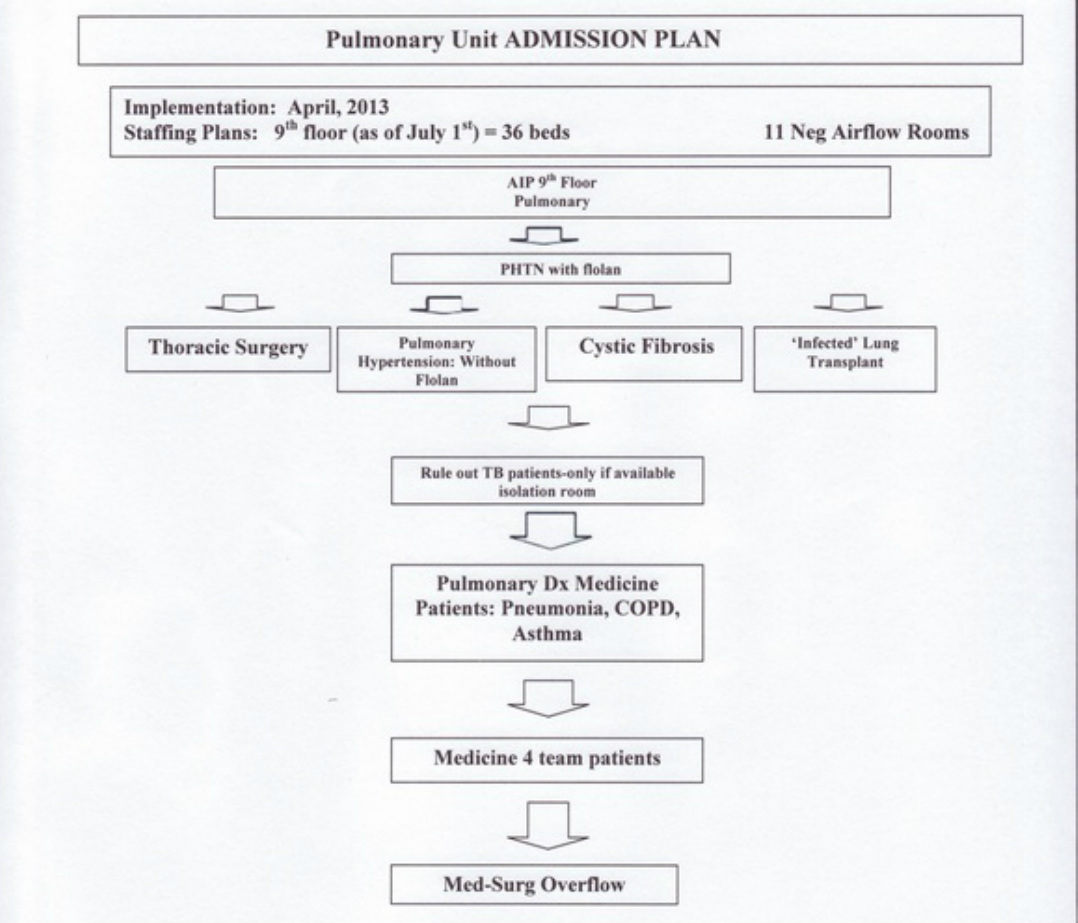
The Pulmonary Unit Admission Plan document prioritizes the order of
patient admissions to the unit. For example, the pulmonary hypertension
(Phtn) patient with a continuous Flolan medication infusion is our number one priority for admission because it is listed towards the top of the document. As the arrows are followed down the document to the Med-Surg overflow at the bottom, this would be our least priority for admission. All the patient types listed above Med-Surg overflow would be a higher priority for admission to the Pulmonary Unit.
patient admissions to the unit. For example, the pulmonary hypertension
(Phtn) patient with a continuous Flolan medication infusion is our number one priority for admission because it is listed towards the top of the document. As the arrows are followed down the document to the Med-Surg overflow at the bottom, this would be our least priority for admission. All the patient types listed above Med-Surg overflow would be a higher priority for admission to the Pulmonary Unit.
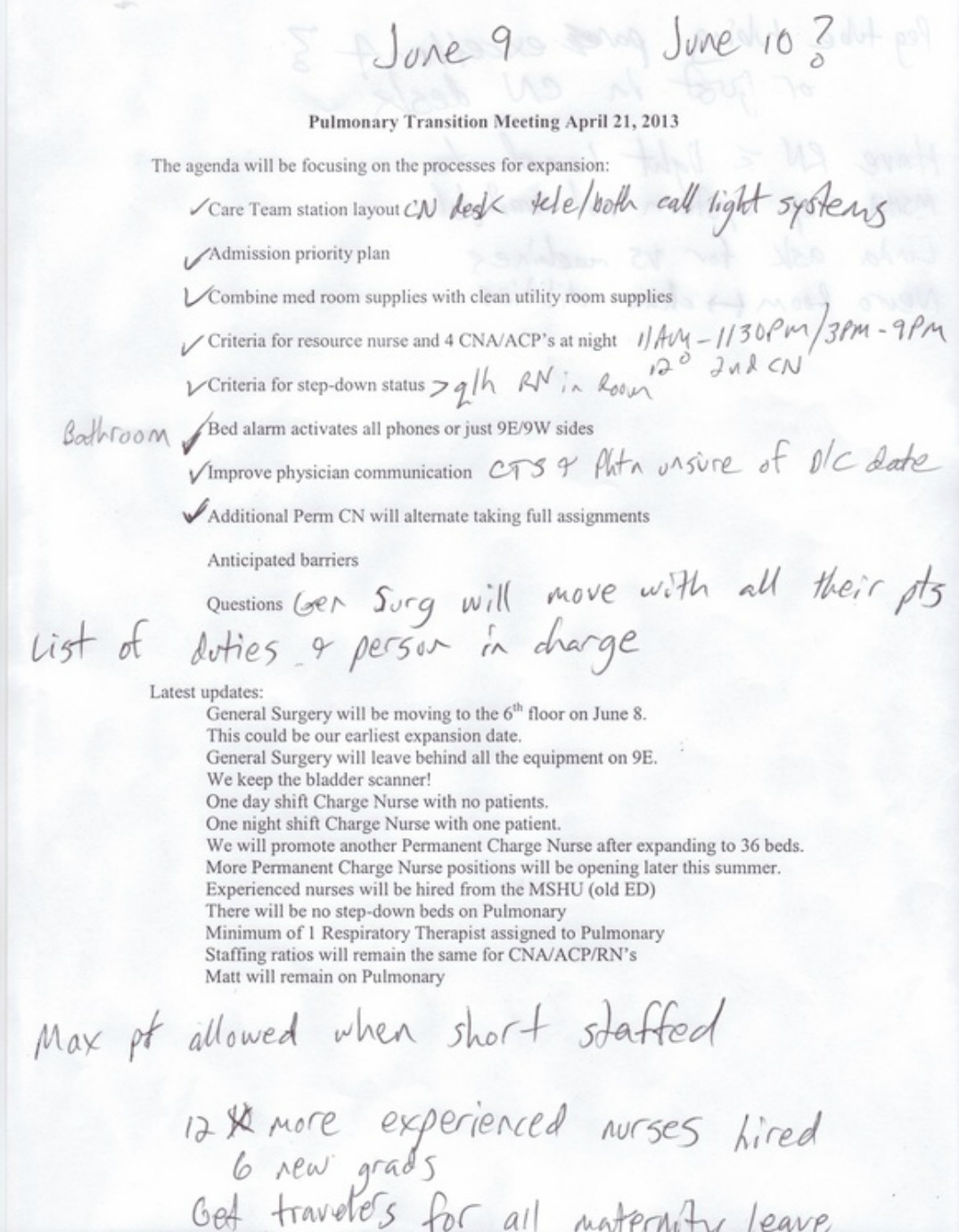
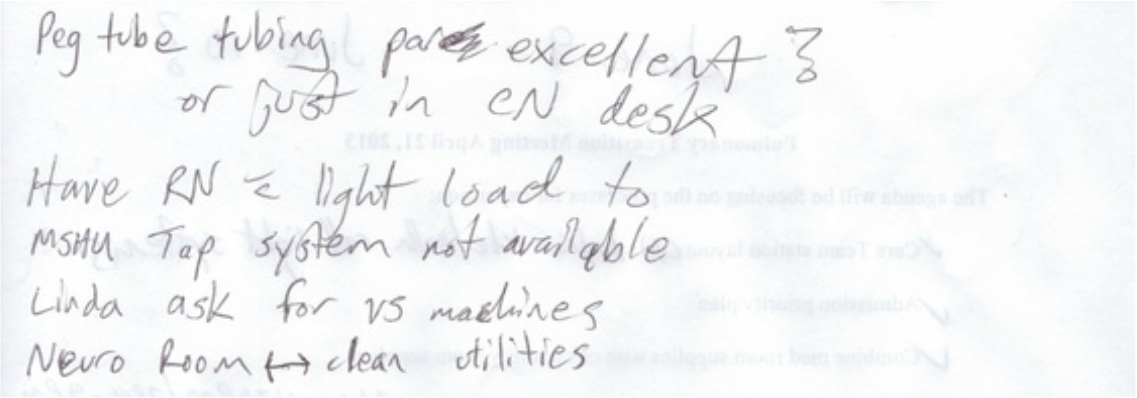
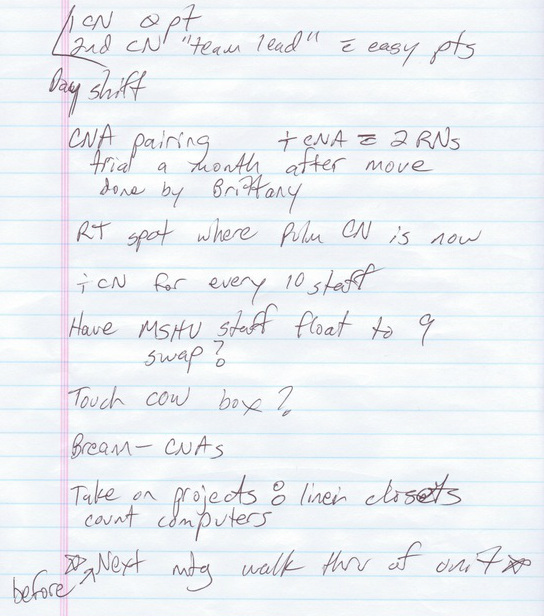
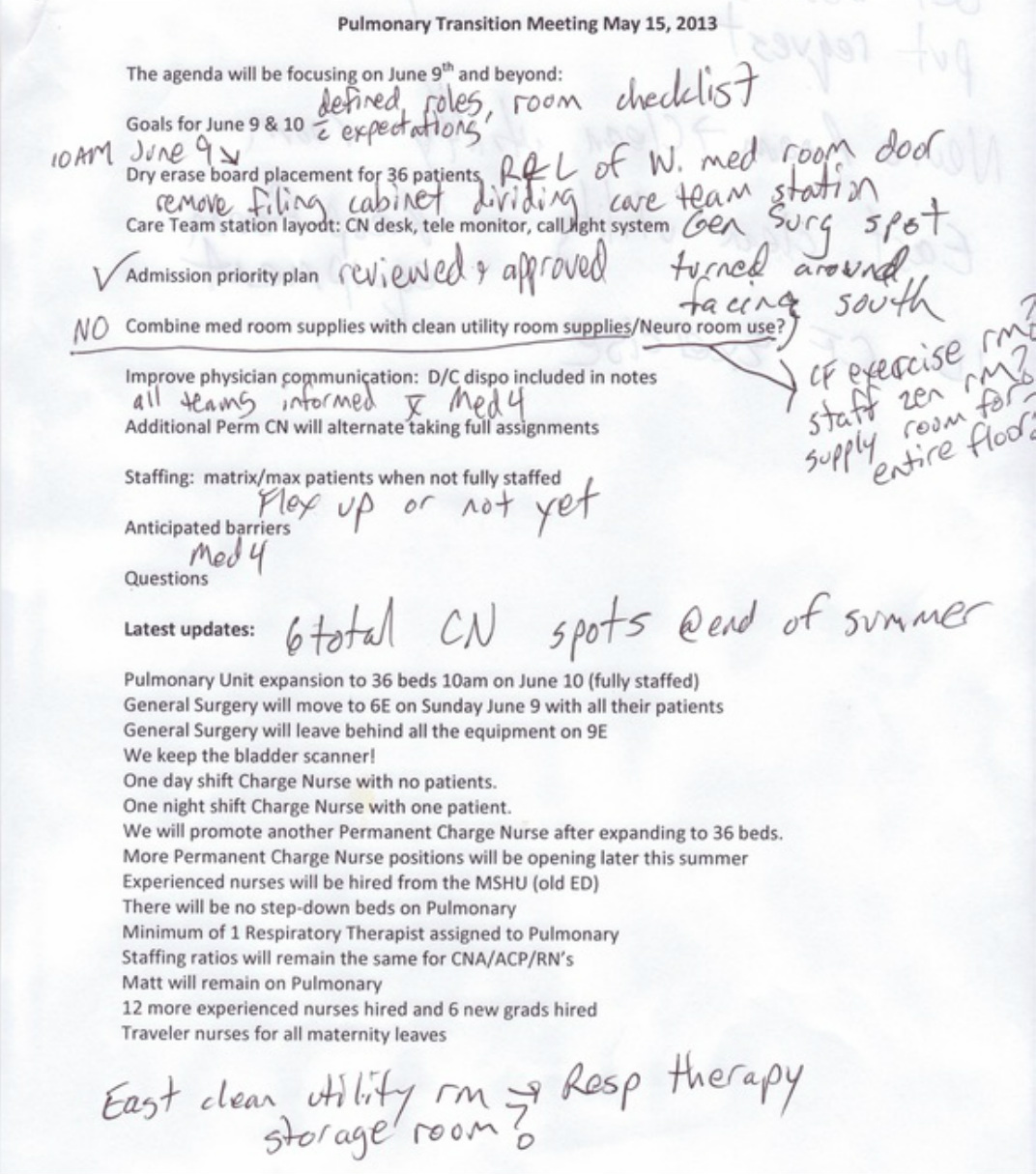
This meeting focused on processes for expansion and was attended by the Pulmonary Unit Manager, Kaycee. At this meeting we discussed the staffing matrix and the potential layouts for the care team station on the backyard deck of my house and enjoyed another potluck meal. The latest updates were discussed along with the names of the experienced nurses that were recently hired. We problem solved the issue of physician communication. I was tasked with several projects: designation of roles for transition day with specific expectations, complete detailed patient room checklists, equipment inventory, supply room organization, and a complete checklist of all duties to be performed on transition day.
The discussion also revealed a change of terminology and process. The terms "open staffed beds" and "staffing matrix" were going away and being replaced with the terms "flexing up." This notion is the responsibility of the Charge Nurse to determine if the unit is safe enough and if the staff are capable of accepting extra patients. The goal is one nurse for every four patients during the day and one nurse for every five patients at night with the term "flex up" designating to go beyond those staffing ratios. The Charge Nurse must assess if the unit can handle extra patients admissions, even if everyone already has a full patient assignment. If the Charge Nurse deems the unit as a whole is unable to accept patients, then this information is communicated to the Hospital Manager as a "flex down" that means the unit is unable to accept patient admissions at this time. The Charge Nurse must be keenly aware that they must prepare the unit to "flex up" if the needs of the hospital dictate as such.
The information from this meeting was disseminated to staff in email form. The Pulmonary Unit website was update with all the latest information. Discussions on the unit continued as our expansion day quickly approached. As the lead of the transition task force, I continued to be a major player in those discussions and continued to collect information via verbal communication, email, phone conversations, and text messages.
Three weeks before the actual transition date, we held the final transition meeting at a nurse's house. After several hours of discussion, we decided to conclude the meeting because the general consensus was that the conversing could go on forever. Below is the email invite, the agenda, and the attendance record. The meeting packet also included the admission plan and the survey results that are not included below because they were previously listed under this tab.
The discussion also revealed a change of terminology and process. The terms "open staffed beds" and "staffing matrix" were going away and being replaced with the terms "flexing up." This notion is the responsibility of the Charge Nurse to determine if the unit is safe enough and if the staff are capable of accepting extra patients. The goal is one nurse for every four patients during the day and one nurse for every five patients at night with the term "flex up" designating to go beyond those staffing ratios. The Charge Nurse must assess if the unit can handle extra patients admissions, even if everyone already has a full patient assignment. If the Charge Nurse deems the unit as a whole is unable to accept patients, then this information is communicated to the Hospital Manager as a "flex down" that means the unit is unable to accept patient admissions at this time. The Charge Nurse must be keenly aware that they must prepare the unit to "flex up" if the needs of the hospital dictate as such.
The information from this meeting was disseminated to staff in email form. The Pulmonary Unit website was update with all the latest information. Discussions on the unit continued as our expansion day quickly approached. As the lead of the transition task force, I continued to be a major player in those discussions and continued to collect information via verbal communication, email, phone conversations, and text messages.
Three weeks before the actual transition date, we held the final transition meeting at a nurse's house. After several hours of discussion, we decided to conclude the meeting because the general consensus was that the conversing could go on forever. Below is the email invite, the agenda, and the attendance record. The meeting packet also included the admission plan and the survey results that are not included below because they were previously listed under this tab.
The final transition meeting covered all the agenda points and provoked much thought on my part. The transition day is closing in quickly and there is so many responsibility that I must complete. Upon reflection, these meetings were a great source of inspiration and a grand collection of information which will revolutionize the Pulmonary Unit. The infrequent interruptions by the staff's children served as a gentle reminder to tone down the rhetoric and refocus on the current topic of discussion. The children and significant others also concocted a sense of reality and comfort that really opened the floodgates of creativity and thought provocation. It was also great to meet several of my coworker's significant others and converse with them on issues outside of the hospital to keep the "shop talk" in check. The whole no dress code atmosphere and off campus location really created an openness where all ideas were heard with out any thought of repercussions.
Final preparation day
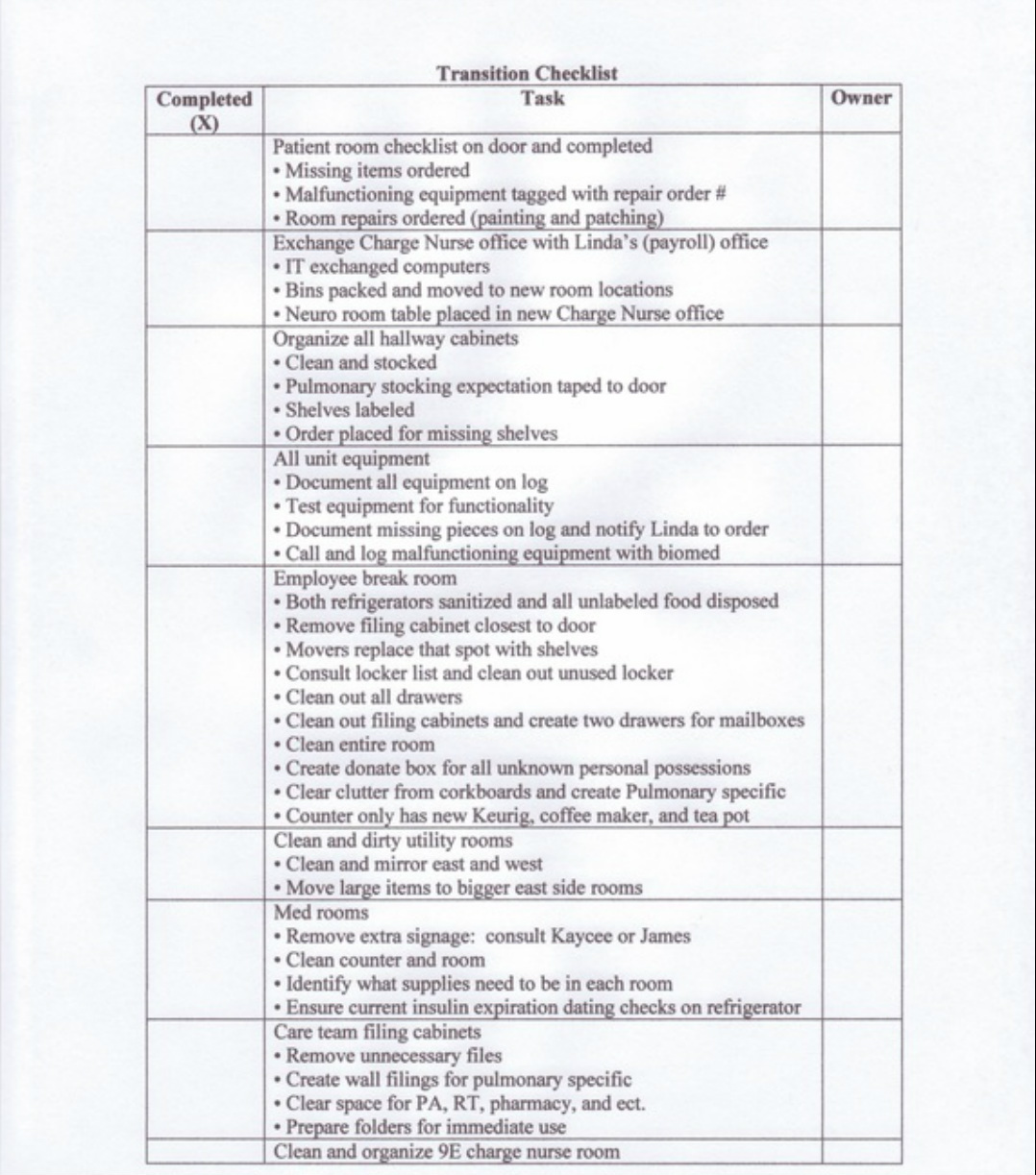
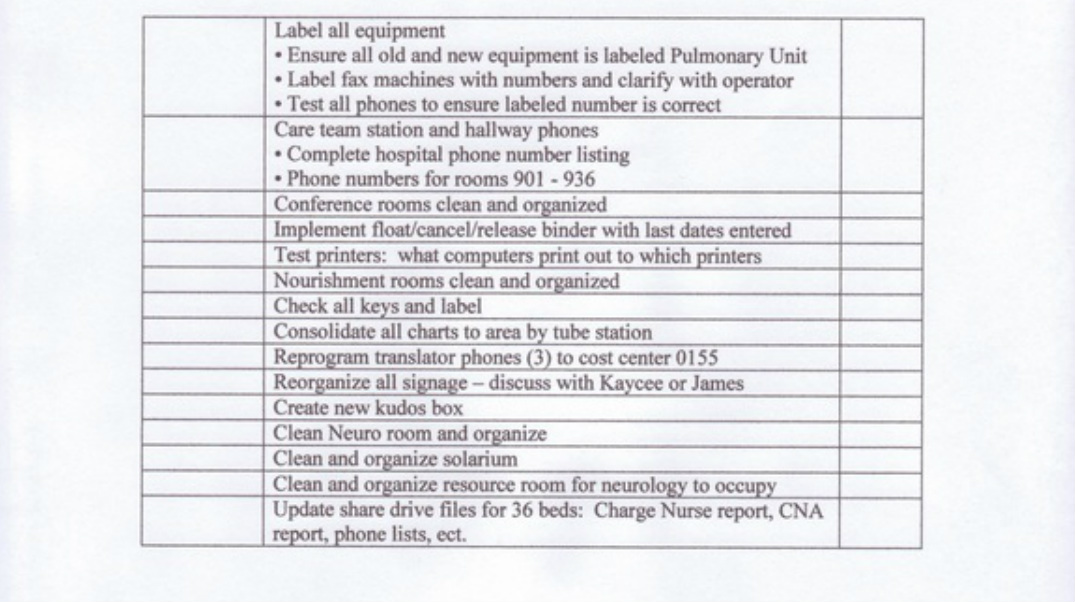
Listed below are the documents that were utilized on this final preparation day. They consist of the Room Checklist, Equipment Log, Patient Room Summary Checklist, and the Transition Checklist .
Final preparation day
Listed below are the documents that were utilized on this final preparation day. They consist of the Room Checklist, Equipment Log, Patient Room Summary Checklist, and the Transition Checklist .
Room Checklist
Room#________
___Hand hygiene sign on door
___Functioning hand sanitizer outside room
___Clear plastic signage containers on door that are not broken
___Made bed functioning properly with pillow and scale zeroed
___Two pillows in closet
___Chair
___Couch
___Night stand
___Call light
___Table
___Clock
___Sharps container
___Small, medium, and large gloves labeled on dispenser
___Phone
___TV
___Trash - large in patient room
___Trash - small in bathroom
___Trash - red biohazard bin
___Curtain in room
___Curtain in bathroom
___Paper towel dispenser with paper towels
___MET sheet attached to paper towel dispenser
___Dry erase board with dry erase pen
___Soap dispensers by both sinks
___Call don't fall sign on wall
___Hair dryer
___Wall suction unit attached and functioning
___Canister ring
___Basket above bed
___Two oxygen meters
___Pulmonary Unit binder
___Remove all extra supplies (tape, IV/blood draw supplies, VHS tapes, ect.)
___Room clean and organized
___Computer and scanner functioning properly
___Call in work orders for painting, patching, and other repairs
Room#________
___Hand hygiene sign on door
___Functioning hand sanitizer outside room
___Clear plastic signage containers on door that are not broken
___Made bed functioning properly with pillow and scale zeroed
___Two pillows in closet
___Chair
___Couch
___Night stand
___Call light
___Table
___Clock
___Sharps container
___Small, medium, and large gloves labeled on dispenser
___Phone
___TV
___Trash - large in patient room
___Trash - small in bathroom
___Trash - red biohazard bin
___Curtain in room
___Curtain in bathroom
___Paper towel dispenser with paper towels
___MET sheet attached to paper towel dispenser
___Dry erase board with dry erase pen
___Soap dispensers by both sinks
___Call don't fall sign on wall
___Hair dryer
___Wall suction unit attached and functioning
___Canister ring
___Basket above bed
___Two oxygen meters
___Pulmonary Unit binder
___Remove all extra supplies (tape, IV/blood draw supplies, VHS tapes, ect.)
___Room clean and organized
___Computer and scanner functioning properly
___Call in work orders for painting, patching, and other repairs
Patient Room Checklist Summary
Cross out room number upon completion (no issues) Issues in progress
901
902
903
904
905
906
907
908
909
910
911
912
913
914
915
916
917
918
919
920
921
922
923
924
925
926
927
928
929
930
931
932
933
934
935
936
Cross out room number upon completion (no issues) Issues in progress
901
902
903
904
905
906
907
908
909
910
911
912
913
914
915
916
917
918
919
920
921
922
923
924
925
926
927
928
929
930
931
932
933
934
935
936
Transition day
The much anticipated day was finally here. Many fellow staff members had come to the hospital to assist with the transition. We reviewed the Transition Checklist document and I accepted volunteers to complete the tasks. The General Surgery Unit began to move patients and we taped a copy of the Room Checklist form to the door of each vacated room. The form would be given to me upon completion of each room and I would update the Patient Room Checklist Summary document to track overall progress. The entire 9th floor was a flurry of people reorganizing, moving, and cleaning.
I managed all the workflows and ensured that all the extra staff had some function to perform. All the equipment was labeled and tested. The entire inventory was documented on the Equipment Log and missing parts were ordered. Malfunctioning equipment was labeled with repair orders placed. We moved everything that we could to give the entire unit a fresh look. Storage cabinets, offices, and supply rooms were cleaned out and reorganized. We worked around painters, maintenance staff, and the people hired by the hospital to move boxes, crates and all other items necessary. I updated the staffing log before General Surgery took their staffing log with them. Eight to nine hours later nearly every item on the Transition Checklist was completed. The move of General Surgery and their patients had only taken a couple of hours.
Expansion day
The east side of the Pulmonary Unit had 18 empty patient rooms. The final work orders were being completed and a few rooms were still being painted. I utilized the Patient Room Checklist Summary one last time to double check each room by performing a personal walk through to ensure that it was ready to receive patients. About 10% of the rooms were not ready to accept patient admissions. The west side of the Pulmonary Unit was business as usual with a patient in every room. Once again, our team came together and were ready to accept admissions. Numerous staff had volunteered to assist with the expansion.
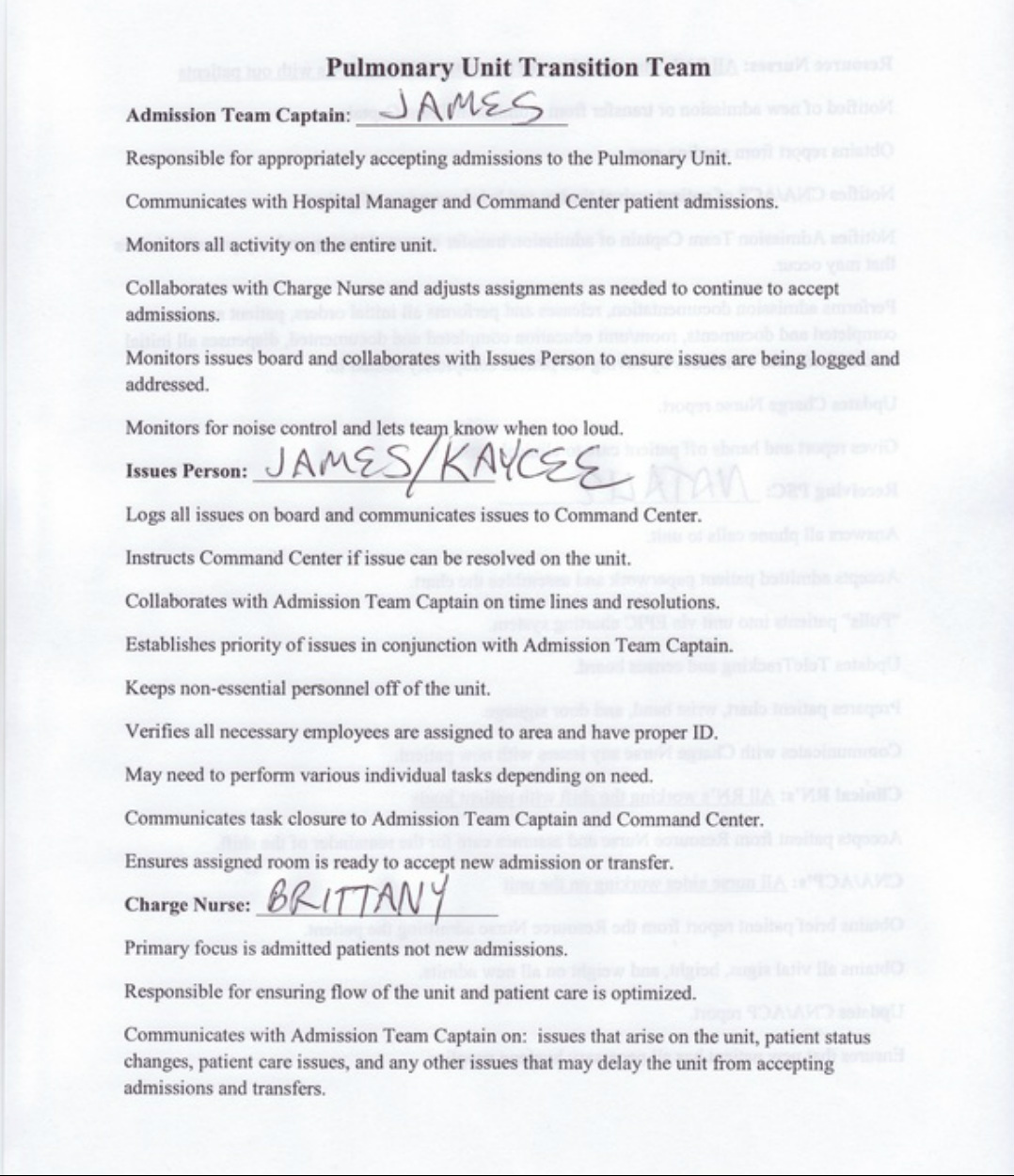
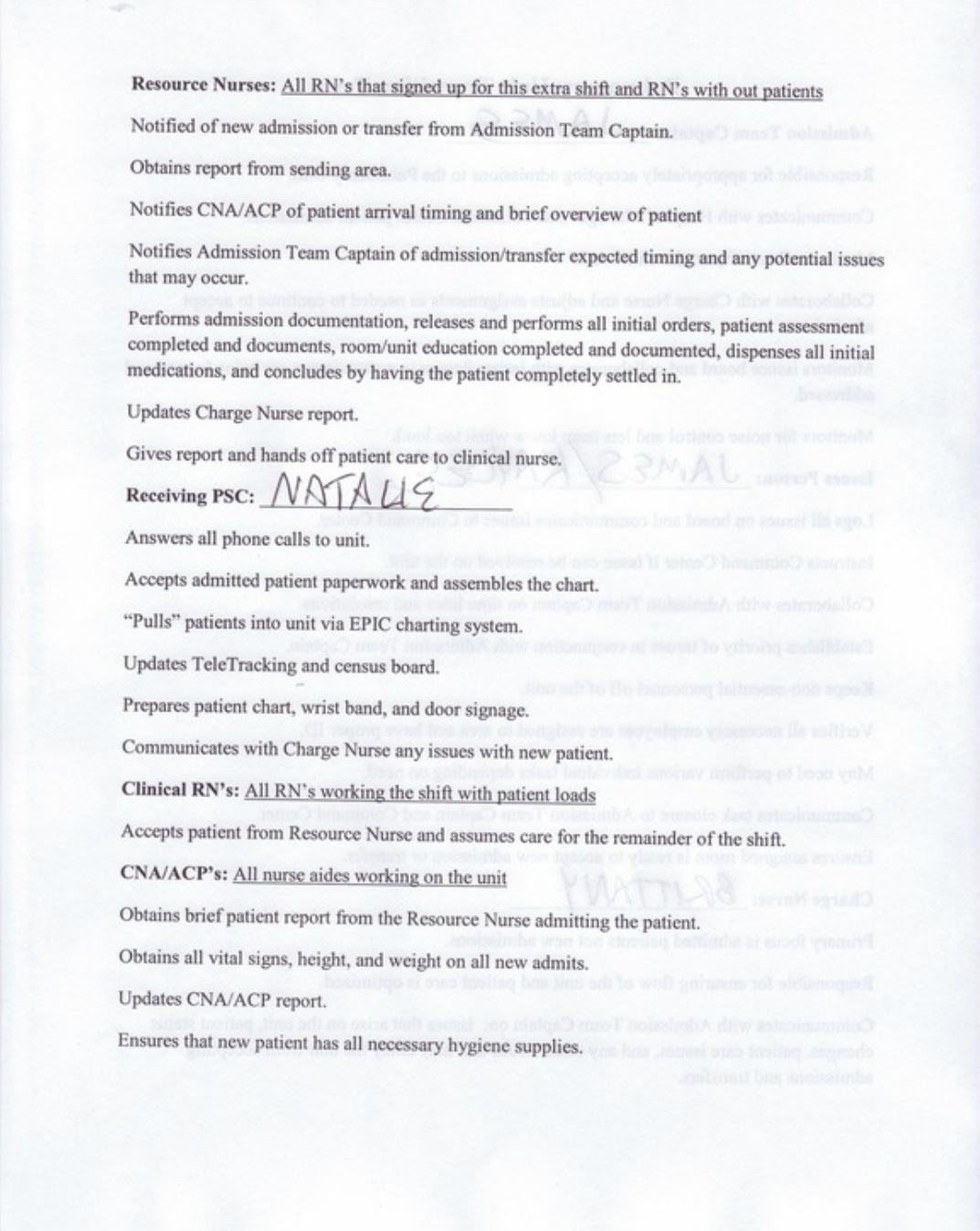
We reviewed the Pulmonary Unit Transition Team document I created for that specific day. This form defined each role and highlighted the expectations for each position. Individual assignments were established. Everyone was ready and we all agreed that the time has come to move forward. I notified the Command Center that we were ready for the first admit.
Telephone report was provided to one of the resource nurses for the first patient on the east side of the Pulmonary Unit. The resource nurse and aide went down to the Emergency Department (ED) to retrieve the patient. I called the Command Center as the patient arrived in our room. Three of the internal transfers we had expected did not occur for various reasons. The Command Center notified me that our next admission was coming from the ED and there were no more admissions left in the ED. I chose the next admission team consisting of another resource nurse and aide to receive report and retrieve the patient. I notified the Command Center of the second patient arrival. The Command Center and the Pulmonary Unit were both satisfied with the progress and it was deemed to be business as usual. This meant the Command Center was signing off on the transition and would only continue to be available for process issues. Below are the team assignments with expectations that were utilized during the expansion day.
Months of preparation had really paid off. The actual admission portion of the transition had taken just over one hour. The efforts and dedication of the entire Pulmonary Unit team was truly amazing. The first day of the Pulmonary Unit transition had gone as planned with no difficulties. The entire unit was reorganized, completely revolutionized, and fully operational.
The entire process converted my perceived position of a coworker to a leader. Actions that were once performed with little thought, now were produced with a more complex understanding of potential implications for each and every action. I truly had a vested interest in the Pulmonary Unit. Ownership of a shift as the Charge Nurse has been transposed to ownership of the daily workings of the entire unit.
The entire process converted my perceived position of a coworker to a leader. Actions that were once performed with little thought, now were produced with a more complex understanding of potential implications for each and every action. I truly had a vested interest in the Pulmonary Unit. Ownership of a shift as the Charge Nurse has been transposed to ownership of the daily workings of the entire unit.