Outcome Initiatives
Contents
Introduction
Teaching activity evaluation
1. Literature review
2. Graph
3. Test questions with data
4. Follow up
Focus-PDCA
1. Literature review
2. Raw data
3. Graph A
4. Graph B
5. Follow up
6. Audit
Introduction
The data was collected to evaluate the teaching activity based on the results of the pretest and the posttest. The data displays how significant levels of learning occurred as a result of the educational sessions. The teaching activity was educating the Pulmonary Unit nursing staff on the Nursing Practice Guideline: Independent Double Check of Medications. The second part of this section highlights the evaluation of the Focus-PDCA. In a three week period in June to July of 2013 the Pulmonary Unit had an increase in the amount of patient falls. 6 patient falls in three weeks required me to come up with a plan to educate the entire unit on the expectations of fall prevention measures.
Teaching activity evaluation
1. Literature review
Dickinson, A., McCall, E., Twomey, B., & James, N. (2010). Paediatric nurses’ understanding of the process and procedure of double-checking medications. Journal of Clinical Nursing. 19: 728-735. (LOE VI)
Hodgkinson, B., Koch, S., Nay, R., & Nichols, K. (2006). Strategies to reduce medication errors with reference to older adults. International Journal
of Evidence Based Healthcare. 4: 2-41. (LOE V)
The Joint Commission. (2008). Preventing errors related to commonly used
anticoagulants. Sentinel Event Alert. 41: 1-3. (LOE VI)
Just, S., Schepers, G., Piotrowski, M., Saint, S., & Kauffman, C. (2006). Improving safety of intravenous admixtures: Lessons learned from a Pentostam overdose. Journal on Quality and Patient Safety. 32(7): 366-372. (LOE V)
Sheu, S., Wei, I., Chen, C., Yu, S., & Tang, F. (2008). Using snowball sampling
method with nurses to understand medication administration errors.
Journal of Clinical Nursing. 18: 559-569. (LOE V)
Smetzer, J. L., & Cohen, M. R. (2007). Preventing drug administration
errors. Medication Errors. 2nd ed., 421-423. (LOE VI)
Starkey, S., & Walden, P. (2010). How do we prevent medication errors? Nursing Made Incredibly Easy. 8 (6): 18-22. (LOE VI)
2. Graph
Contents
Introduction
Teaching activity evaluation
1. Literature review
2. Graph
3. Test questions with data
4. Follow up
Focus-PDCA
1. Literature review
2. Raw data
3. Graph A
4. Graph B
5. Follow up
6. Audit
Introduction
The data was collected to evaluate the teaching activity based on the results of the pretest and the posttest. The data displays how significant levels of learning occurred as a result of the educational sessions. The teaching activity was educating the Pulmonary Unit nursing staff on the Nursing Practice Guideline: Independent Double Check of Medications. The second part of this section highlights the evaluation of the Focus-PDCA. In a three week period in June to July of 2013 the Pulmonary Unit had an increase in the amount of patient falls. 6 patient falls in three weeks required me to come up with a plan to educate the entire unit on the expectations of fall prevention measures.
Teaching activity evaluation
1. Literature review
Dickinson, A., McCall, E., Twomey, B., & James, N. (2010). Paediatric nurses’ understanding of the process and procedure of double-checking medications. Journal of Clinical Nursing. 19: 728-735. (LOE VI)
Hodgkinson, B., Koch, S., Nay, R., & Nichols, K. (2006). Strategies to reduce medication errors with reference to older adults. International Journal
of Evidence Based Healthcare. 4: 2-41. (LOE V)
The Joint Commission. (2008). Preventing errors related to commonly used
anticoagulants. Sentinel Event Alert. 41: 1-3. (LOE VI)
Just, S., Schepers, G., Piotrowski, M., Saint, S., & Kauffman, C. (2006). Improving safety of intravenous admixtures: Lessons learned from a Pentostam overdose. Journal on Quality and Patient Safety. 32(7): 366-372. (LOE V)
Sheu, S., Wei, I., Chen, C., Yu, S., & Tang, F. (2008). Using snowball sampling
method with nurses to understand medication administration errors.
Journal of Clinical Nursing. 18: 559-569. (LOE V)
Smetzer, J. L., & Cohen, M. R. (2007). Preventing drug administration
errors. Medication Errors. 2nd ed., 421-423. (LOE VI)
Starkey, S., & Walden, P. (2010). How do we prevent medication errors? Nursing Made Incredibly Easy. 8 (6): 18-22. (LOE VI)
2. Graph
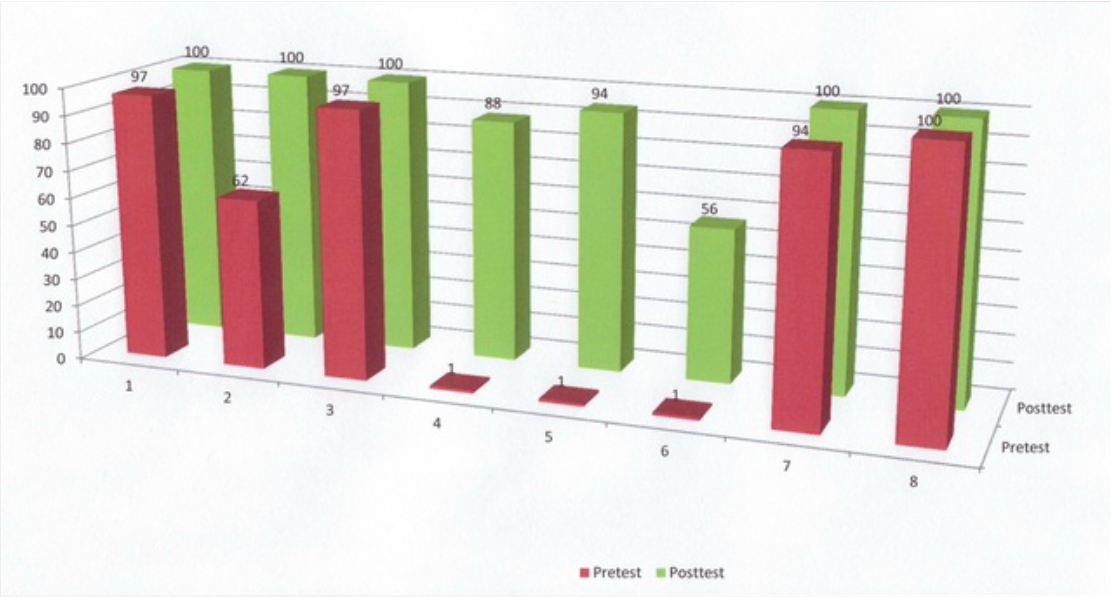
The teaching activity had a pretest to evaluate the current level of understanding before education had taken place. The results of the pretest in percentage of correct answers are listed in the color red on the graph. A posttest was taken at the conclusion of the education exercise. The results of the posttest in percentage of correct answers are listed on the graph in the color green. The base of the graph is numbered 1-8 to indicate the corresponding question taken from the pretest and posttest. The questions were the same on both tests to minimize extraneous variables that could jeopardize the results of the experiment. The size of the sample is 34 nurses (n=34).
3. Test questions with data
1. True or false? Care handoff is defined as any situation where another Healthcare Personnel assumes the care of the patient for the remainder of the shift, accepting a patient transferred from another area of the organization, or at the change of shift.
_X_True ___False
Pretest 97% correct Posttest 100% correct
This is care handoff as defined in the guideline.
2. True or false? All IV medications that are deemed high risk may be documented under the EPIC care handoff communication tab of “IV lines & drips
reviewed”.
___True _X_False
Pretest 62% correct Posttest 100% correct
All medications may be documented in this fashion except high risk medications. High risk medications must be documented in the Medication Administration Record (MAR) with the dual signoff format.
3. True or false? An independent double check of a medication is defined as two RN’s separately verify the medication, volume, concentration, and rate, then authenticate all the information with the Medication Administration Record (MAR) to reach the same conclusion.
_X_True ___False
Pretest 97% correct Posttest 100% correct
This is defined in the guideline and highlights the actual expectation of an independent double check.
4. Which of the following IV medications would require an independent
double check and EPIC cosign when care handoff has taken place?
Check all that apply.
___Cytogam _X_Insulin ___Synagist
_X_Argatroban _X_Rituximab ___Thymoglobulin
___Lasix ___Solumedrol _X_Magnesium (20gm)
_X_Bivalirudin _X_Remodulin _X_PCA/PCEA
_X_Chemotherapy _X_Flolan ___Magnesium (1-2gm)
_X_Heparin ___Potassium ___IVIG
Pretest 1% correct Posttest 88% correct
This question emphasizes which medications are deemed high risk and the care handoff expectation.
5. Which of the following IV medications would require an independent
double check and EPIC cosign when a bolus dose is given?
Check all that apply.
___Cytogam _X_Insulin ___Synagist
_X_Argatroban ___Rituximab ___Thymoglobulin
___Lasix ___Solumedrol ___Magnesium (20gm)
_X_Bivalirudin ___Remodulin _X_PCA/PCEA
___Chemotherapy ___Flolan ___Magnesium(1-2gm)
_X_Heparin ___Potassium ___IVIG
Pretest 1% correct Posttest 94% correct
This question highlights the importance of double checking before a bolus dose is given and which medications the bolus function is performed. A bolus is large dose of the medication infused rapidly.
6. Which of the following IV medications would require an independent
double check and EPIC cosign when a rate change is performed?
Check all that apply.
___Cytogam ___Insulin ___Synagist
_X_Argatroban ___Rituximab ___Thymoglobulin
___Lasix ___Solumedrol _X_Magnesium(20gm)
_X_Bivalirudin _X_Remodulin _X_PCA/PCEA
_X_Chemotherapy _X_Flolan ___Magnesium(1-2gm)
_X_Heparin ___Potassium ___IVIG
Pretest 1% correct Posttest 56% correct
This question differentiates which medications require an independent double check when the rate is changed. Many nurses also selected insulin on the posttest, for this practice is routinely performed on the Pulmonary Unit even though it is not a component of the Nursing Practice Guideline.
7. Which of the following IV medications would require an independent
double check and EPIC cosign when a dosage change is performed?
Check all that apply.
___Cytogam ___Insulin ___Synagist
___Argatroban ___Rituximab ___Thymoglobulin
___Lasix ___Solumedrol ___Magnesium(20gm)
___Bivalirudin _X_Remodulin _X_PCA/PCEA
___Chemotherapy _X_Flolan ___Magnesium(1-2gm)
___Heparin ___Potassium ___IVIG
Pretest 94% correct Posttest 100% correct
These medications emphasize the importance of an independent double check to ensure the infusion dosage matches what is listed in the MAR. Most medications have only one standard dose in the hospital setting.
8. Where would you find the policy/procedure/guideline on the
administration of high risk IV
medications?__________________________________________________
Everyone answered this question correctly on the pretest and posttest. The
hospital's website known as the HUB is the place everyone goes to for the most
recent information on policies, procedures, and guidelines.
4. Follow up
I will continue to be a resource for this Nursing Practice Guideline for my unit and all Medical-Surgical areas of the hospital. Documentation audits will continue on my unit to ensure compliance. The audits will reveal which staff members require more in-depth education. I am currently working with Managers and Educators to disseminate the expectations of the guideline to all Medical-Surgical areas of the hospital.
Focus-PDCA
During a three week period in June to July of 2013 the Pulmonary Unit witnessed a significant increase in the amount of patient falls. The unit usually goes months with out a single patient fall but this three week period had 6 patient falls. I performed a Focus-PDCA to determine what factors contributed to the increase in patients falling. Several variables were isolated as a result of staff interviews, documentation assessments, and random audits of fall prevention measures. There were many inconsistencies with fall prevention measures correlating to the patients that were assessed to be a high fall risk. Random audits have shown that only 50% of high fall risk patients have the bed alarm on which is a requirement based on hospital policy. The actual patient fall documentation revealed that some staff members were not remaining with high fall risk patients while the patient was in the bathroom that had resulted in 2 patient falls. I took it upon myself to educate staff to remedy this situation.
1. Literature review
Lake, E., Shang, J., Klaus. S., & Dunton, N. (2010). Patient falls: Association with hospital magnet status and nursing unit staffing. Resident Nursing Health. 33(5): 413-425. (LOE IV)
Kraft, T. (2013). Hospital achieves 50% reduction in falls. Hospital Case Management. 21(6): 86-88. (LOE VI)
Quigley, P., Neily, J., Watson, M., Wright, M., & Strobel, K. (2007). Measuring fall program outcomes. The Online Journal of Issues in Nursing. 12(2). (LOE IV)
Shorr, R., Chandler, A., Mion, L., & Waters, T. (2012). Effects of an intervention to increase bed alarm use to prevent falls in hospitalized patients: A cluster of randomized trials. Annals of Internal Medicine. 157(10): 145-153. (LOE II)
2. Raw data
Month Year Number of patient falls
August 2012 0
September 2012 0
October 2012 0
November 2012 2
December 2012 0
January 2013 1
February 2013 0
March 2013 2
April 2013 0
May 2013 1
June 2013 2
July 2013 4
3. Graph A
3. Test questions with data
1. True or false? Care handoff is defined as any situation where another Healthcare Personnel assumes the care of the patient for the remainder of the shift, accepting a patient transferred from another area of the organization, or at the change of shift.
_X_True ___False
Pretest 97% correct Posttest 100% correct
This is care handoff as defined in the guideline.
2. True or false? All IV medications that are deemed high risk may be documented under the EPIC care handoff communication tab of “IV lines & drips
reviewed”.
___True _X_False
Pretest 62% correct Posttest 100% correct
All medications may be documented in this fashion except high risk medications. High risk medications must be documented in the Medication Administration Record (MAR) with the dual signoff format.
3. True or false? An independent double check of a medication is defined as two RN’s separately verify the medication, volume, concentration, and rate, then authenticate all the information with the Medication Administration Record (MAR) to reach the same conclusion.
_X_True ___False
Pretest 97% correct Posttest 100% correct
This is defined in the guideline and highlights the actual expectation of an independent double check.
4. Which of the following IV medications would require an independent
double check and EPIC cosign when care handoff has taken place?
Check all that apply.
___Cytogam _X_Insulin ___Synagist
_X_Argatroban _X_Rituximab ___Thymoglobulin
___Lasix ___Solumedrol _X_Magnesium (20gm)
_X_Bivalirudin _X_Remodulin _X_PCA/PCEA
_X_Chemotherapy _X_Flolan ___Magnesium (1-2gm)
_X_Heparin ___Potassium ___IVIG
Pretest 1% correct Posttest 88% correct
This question emphasizes which medications are deemed high risk and the care handoff expectation.
5. Which of the following IV medications would require an independent
double check and EPIC cosign when a bolus dose is given?
Check all that apply.
___Cytogam _X_Insulin ___Synagist
_X_Argatroban ___Rituximab ___Thymoglobulin
___Lasix ___Solumedrol ___Magnesium (20gm)
_X_Bivalirudin ___Remodulin _X_PCA/PCEA
___Chemotherapy ___Flolan ___Magnesium(1-2gm)
_X_Heparin ___Potassium ___IVIG
Pretest 1% correct Posttest 94% correct
This question highlights the importance of double checking before a bolus dose is given and which medications the bolus function is performed. A bolus is large dose of the medication infused rapidly.
6. Which of the following IV medications would require an independent
double check and EPIC cosign when a rate change is performed?
Check all that apply.
___Cytogam ___Insulin ___Synagist
_X_Argatroban ___Rituximab ___Thymoglobulin
___Lasix ___Solumedrol _X_Magnesium(20gm)
_X_Bivalirudin _X_Remodulin _X_PCA/PCEA
_X_Chemotherapy _X_Flolan ___Magnesium(1-2gm)
_X_Heparin ___Potassium ___IVIG
Pretest 1% correct Posttest 56% correct
This question differentiates which medications require an independent double check when the rate is changed. Many nurses also selected insulin on the posttest, for this practice is routinely performed on the Pulmonary Unit even though it is not a component of the Nursing Practice Guideline.
7. Which of the following IV medications would require an independent
double check and EPIC cosign when a dosage change is performed?
Check all that apply.
___Cytogam ___Insulin ___Synagist
___Argatroban ___Rituximab ___Thymoglobulin
___Lasix ___Solumedrol ___Magnesium(20gm)
___Bivalirudin _X_Remodulin _X_PCA/PCEA
___Chemotherapy _X_Flolan ___Magnesium(1-2gm)
___Heparin ___Potassium ___IVIG
Pretest 94% correct Posttest 100% correct
These medications emphasize the importance of an independent double check to ensure the infusion dosage matches what is listed in the MAR. Most medications have only one standard dose in the hospital setting.
8. Where would you find the policy/procedure/guideline on the
administration of high risk IV
medications?__________________________________________________
Everyone answered this question correctly on the pretest and posttest. The
hospital's website known as the HUB is the place everyone goes to for the most
recent information on policies, procedures, and guidelines.
4. Follow up
I will continue to be a resource for this Nursing Practice Guideline for my unit and all Medical-Surgical areas of the hospital. Documentation audits will continue on my unit to ensure compliance. The audits will reveal which staff members require more in-depth education. I am currently working with Managers and Educators to disseminate the expectations of the guideline to all Medical-Surgical areas of the hospital.
Focus-PDCA
During a three week period in June to July of 2013 the Pulmonary Unit witnessed a significant increase in the amount of patient falls. The unit usually goes months with out a single patient fall but this three week period had 6 patient falls. I performed a Focus-PDCA to determine what factors contributed to the increase in patients falling. Several variables were isolated as a result of staff interviews, documentation assessments, and random audits of fall prevention measures. There were many inconsistencies with fall prevention measures correlating to the patients that were assessed to be a high fall risk. Random audits have shown that only 50% of high fall risk patients have the bed alarm on which is a requirement based on hospital policy. The actual patient fall documentation revealed that some staff members were not remaining with high fall risk patients while the patient was in the bathroom that had resulted in 2 patient falls. I took it upon myself to educate staff to remedy this situation.
1. Literature review
Lake, E., Shang, J., Klaus. S., & Dunton, N. (2010). Patient falls: Association with hospital magnet status and nursing unit staffing. Resident Nursing Health. 33(5): 413-425. (LOE IV)
Kraft, T. (2013). Hospital achieves 50% reduction in falls. Hospital Case Management. 21(6): 86-88. (LOE VI)
Quigley, P., Neily, J., Watson, M., Wright, M., & Strobel, K. (2007). Measuring fall program outcomes. The Online Journal of Issues in Nursing. 12(2). (LOE IV)
Shorr, R., Chandler, A., Mion, L., & Waters, T. (2012). Effects of an intervention to increase bed alarm use to prevent falls in hospitalized patients: A cluster of randomized trials. Annals of Internal Medicine. 157(10): 145-153. (LOE II)
2. Raw data
Month Year Number of patient falls
August 2012 0
September 2012 0
October 2012 0
November 2012 2
December 2012 0
January 2013 1
February 2013 0
March 2013 2
April 2013 0
May 2013 1
June 2013 2
July 2013 4
3. Graph A
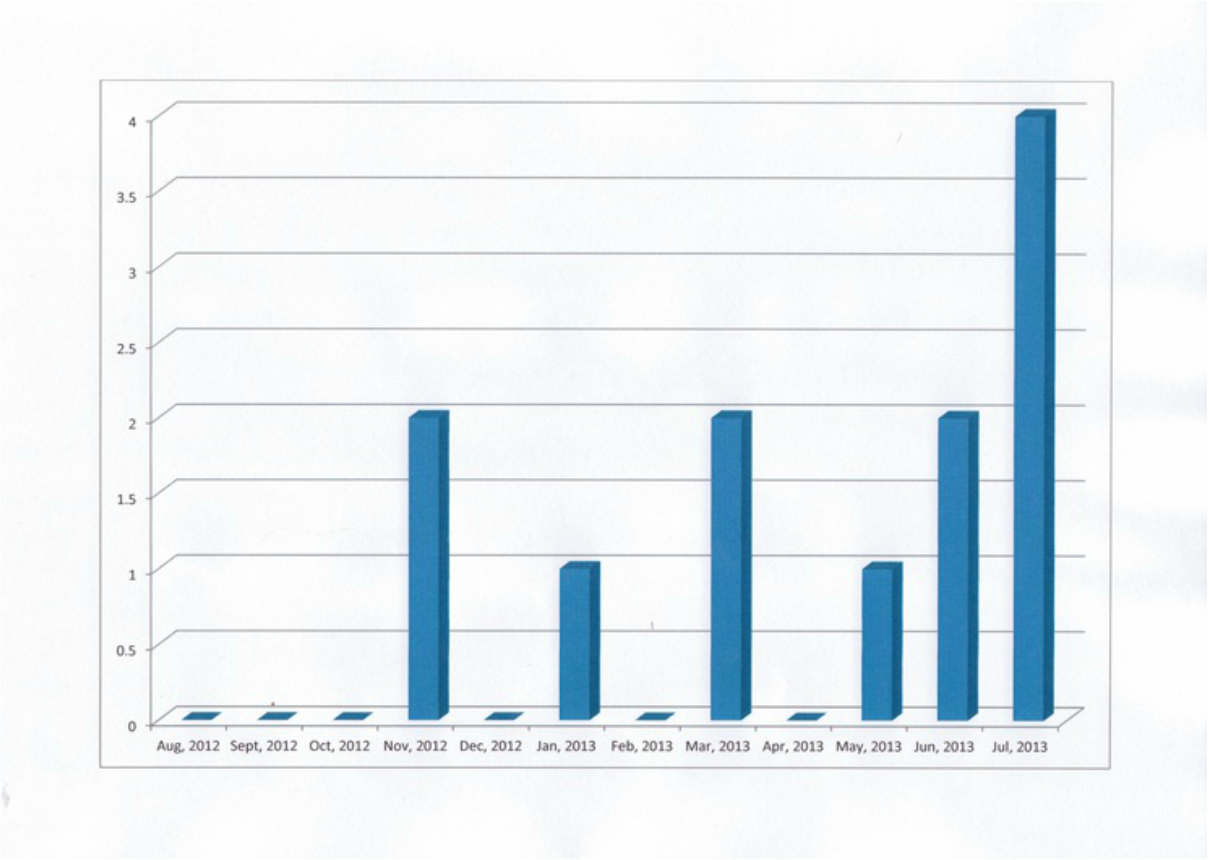
This graph displays the amount of patient falls per month for the past year on the Pulmonary Unit. The chart begins in August of 2012 and concludes on July of 2013. I could not include August of 2013, for the portfolio submission must occur before the actual month is over. The Focus PDCA was created and placed into action in the beginning of July, 2013 due to the rise in patient falls. The staff education on fall prevention measures and expectations continues into August, 2013. The preliminary results of the Focus-PDCA look favorable with no patient falls thus far in the month of August on this the day of August 27, 2013. The last patient fall on the Pulmonary Unit had occurred on July 19, 2013. The true test of the validity of the Focus-PDCA will be displayed over the course of the next six months.
4. Graph B
4. Graph B
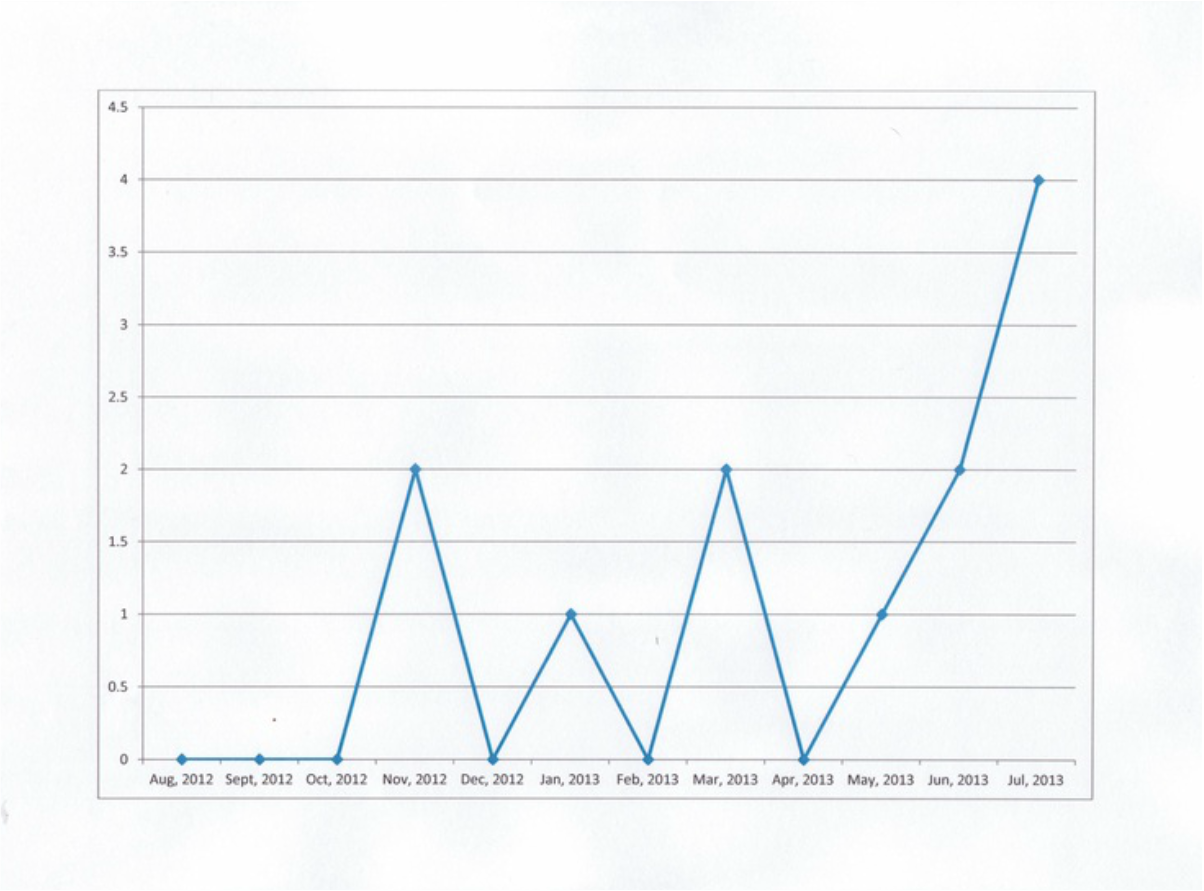
I decided to graph the same information in linear form that displays the trends more visibly. The presentation of information is perceived and
comprehended differently. Some people thrive with raw data. Other people can draw conclusions easily with the data in regular graph form. Linear graphing of data provides a concise line for the eyes to follow that yields deeper understanding in some individuals. All three forms of the data presentation contain the same information. Which one speaks to you?
5. Follow up
I will continue to perform random audits with my Manager to determine where educational opportunities are needed. These audits will also be included in the annual evaluation of each staff member. The last patient fall on the Pulmonary Unit occurred on July 19, 2013. The Focus-PDCA was set into action during the first week of July, 2013. The next six months will determine what the level of effectiveness is for the Focus-PDCA and what changes, if any, are needed to prevent patient falls on the Pulmonary Unit.
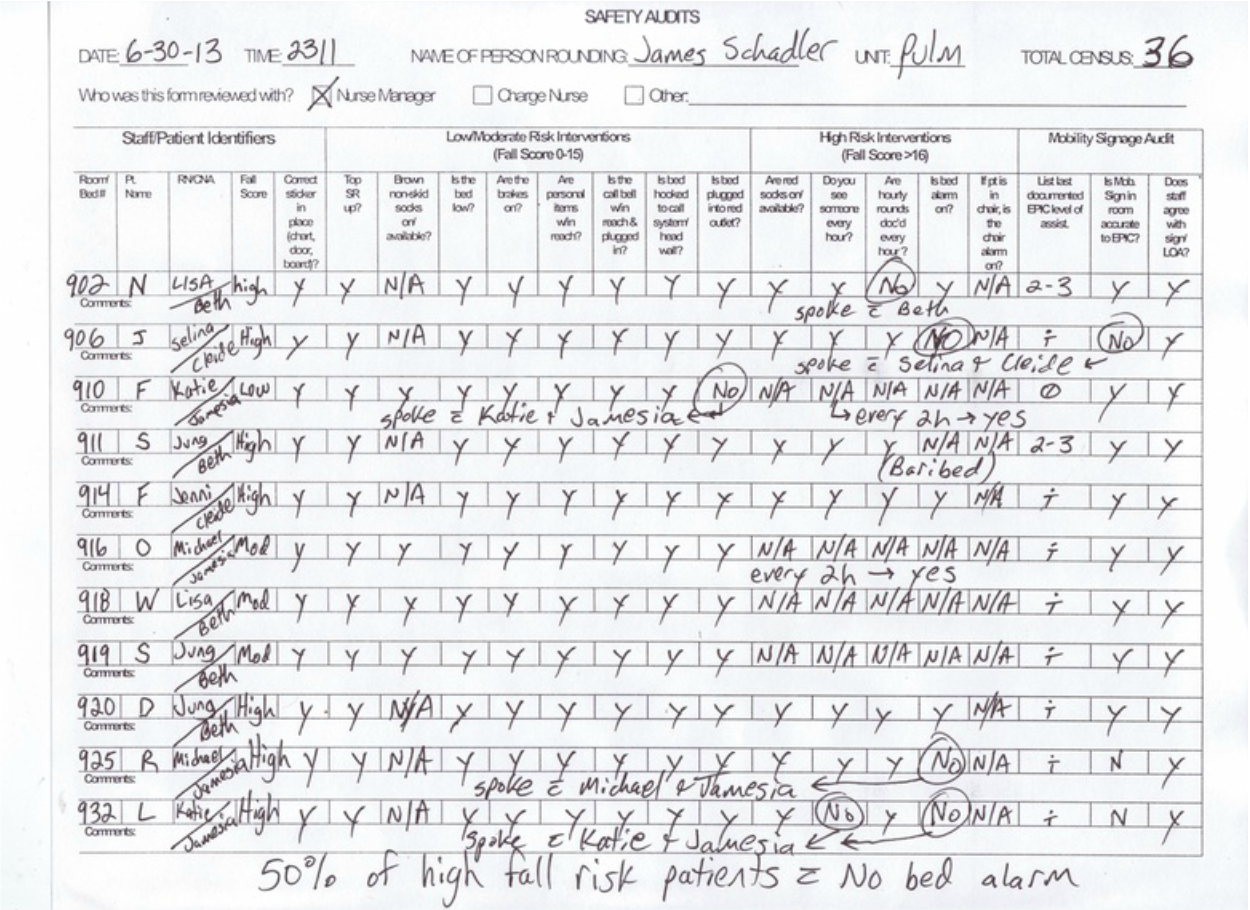
6. Audit
Below is one of the audits that were performed that contributed to the Focus-PDCA. Patients are assessed to determine if their risk of a fall is low, moderate, or high. The fall prevention measures correspond to the patient's fall risk. For example, a patient assessed to be a high fall risk will have all available interventions in place. The audit explores the documented fall risk assessment and tracks what intervention are actually utilized based on visualizing the patient's room for the implementation of each fall prevention measure.
comprehended differently. Some people thrive with raw data. Other people can draw conclusions easily with the data in regular graph form. Linear graphing of data provides a concise line for the eyes to follow that yields deeper understanding in some individuals. All three forms of the data presentation contain the same information. Which one speaks to you?
5. Follow up
I will continue to perform random audits with my Manager to determine where educational opportunities are needed. These audits will also be included in the annual evaluation of each staff member. The last patient fall on the Pulmonary Unit occurred on July 19, 2013. The Focus-PDCA was set into action during the first week of July, 2013. The next six months will determine what the level of effectiveness is for the Focus-PDCA and what changes, if any, are needed to prevent patient falls on the Pulmonary Unit.
6. Audit
Below is one of the audits that were performed that contributed to the Focus-PDCA. Patients are assessed to determine if their risk of a fall is low, moderate, or high. The fall prevention measures correspond to the patient's fall risk. For example, a patient assessed to be a high fall risk will have all available interventions in place. The audit explores the documented fall risk assessment and tracks what intervention are actually utilized based on visualizing the patient's room for the implementation of each fall prevention measure.