Guideline
Contents
Introduction
Literature review
Final draft
Original policy
Revision of policy
1. Drafts
Introduction
It was readily apparent that there was much confusion about which medications required an independent double check and cosign when care handoff was performed at the bedside of the patient. I made it my duty to clarify these issues for all the medical and surgical areas of the hospital. This process began in September of 2012 and concluded in February of 2013. A review of the current literature provided guidance.
Literature review
Dickinson, A., McCall, E., Twomey, B., & James, N. (2010). Paediatric
nurses’ understanding of the process and procedure of double-checking
medications. Journal of Clinical Nursing. 19: 728-735. (LOE VI)
Hodgkinson, B., Koch, S., Nay, R., & Nichols, K. (2006). Strategies to reduce medication errors with reference to older adults. International Journal
of Evidence Based Healthcare. 4: 2-41. (LOE V)
The Joint Commission. (2008). Preventing errors related to commonly used anticoagulants. Sentinel Event Alert. 41: 1-3. (LOE VI)
Just, S., Schepers, G., Piotrowski, M., Saint, S., & Kauffman, C. (2006). Improving safety of intravenous admixtures: Lessons learned from a Pentostam overdose. Journal on Quality and Patient Safety. 32(7): 366-372. (LOE V)
Sheu, S., Wei, I., Chen, C., Yu, S., & Tang, F. (2008). Using snowball sampling
method with nurses to understand medication administration errors. Journal of Clinical Nursing. 18: 559-569. (LOE V)
Smetzer, J. L., & Cohen, M. R. (2007). Preventing drug administration errors. Medication Errors. 2nd ed., 421-423. (LOE VI)
Starkey, S., & Walden, P. (2010). How do we prevent medication errors? Nursing Made Incredibly Easy. 8 (6): 18-22. (LOE VI)
Final draft
This is the actual guideline as it appears on the University of Colorado
Hospital's website, also know as the HUB. The guideline is located by
utilizing the Policy/Procedure/Guideline link.
Contents
Introduction
Literature review
Final draft
Original policy
Revision of policy
1. Drafts
Introduction
It was readily apparent that there was much confusion about which medications required an independent double check and cosign when care handoff was performed at the bedside of the patient. I made it my duty to clarify these issues for all the medical and surgical areas of the hospital. This process began in September of 2012 and concluded in February of 2013. A review of the current literature provided guidance.
Literature review
Dickinson, A., McCall, E., Twomey, B., & James, N. (2010). Paediatric
nurses’ understanding of the process and procedure of double-checking
medications. Journal of Clinical Nursing. 19: 728-735. (LOE VI)
Hodgkinson, B., Koch, S., Nay, R., & Nichols, K. (2006). Strategies to reduce medication errors with reference to older adults. International Journal
of Evidence Based Healthcare. 4: 2-41. (LOE V)
The Joint Commission. (2008). Preventing errors related to commonly used anticoagulants. Sentinel Event Alert. 41: 1-3. (LOE VI)
Just, S., Schepers, G., Piotrowski, M., Saint, S., & Kauffman, C. (2006). Improving safety of intravenous admixtures: Lessons learned from a Pentostam overdose. Journal on Quality and Patient Safety. 32(7): 366-372. (LOE V)
Sheu, S., Wei, I., Chen, C., Yu, S., & Tang, F. (2008). Using snowball sampling
method with nurses to understand medication administration errors. Journal of Clinical Nursing. 18: 559-569. (LOE V)
Smetzer, J. L., & Cohen, M. R. (2007). Preventing drug administration errors. Medication Errors. 2nd ed., 421-423. (LOE VI)
Starkey, S., & Walden, P. (2010). How do we prevent medication errors? Nursing Made Incredibly Easy. 8 (6): 18-22. (LOE VI)
Final draft
This is the actual guideline as it appears on the University of Colorado
Hospital's website, also know as the HUB. The guideline is located by
utilizing the Policy/Procedure/Guideline link.
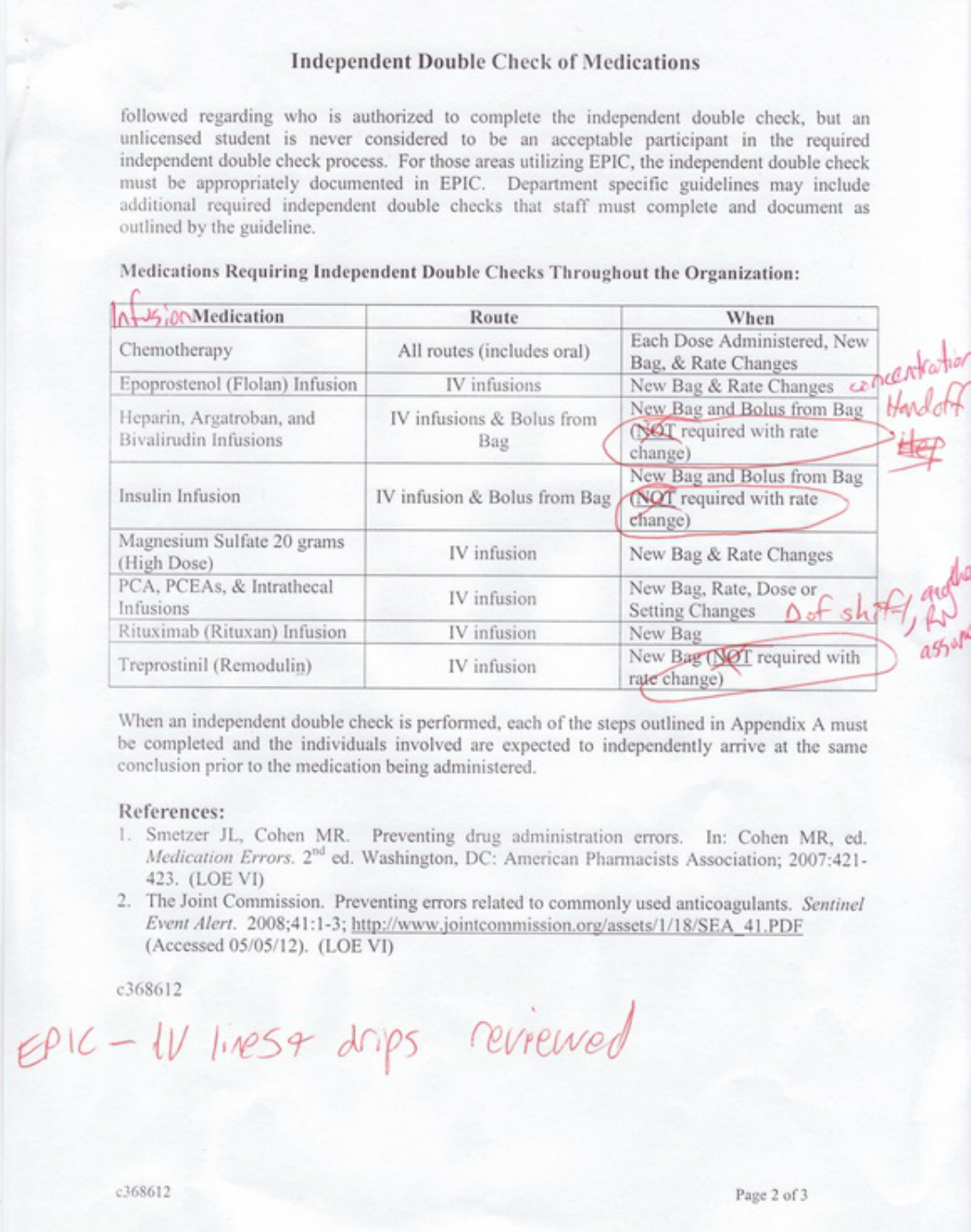
Original policy
Revision of policy
The unit educator and I were reviewing the policy shown above, that directly affected the Pulmonary Unit. The Independent Double Check of High Risk Medications Policy did not require an independent double check of dose changes for Epoprostenol (Flolan) and Treprostinil (Remodulin). The administration and monitoring of these medications are one of the specialties of the Pulmonary Unit. It is routine practice to independently double check and cosign all dosage changes with two Registered Nurses (RN) of this medication that treats pulmonary hypertension with a continuous infusion through a pump that looks similar to the traditional Patient Controlled Analgesia (PCA) pump but has significant differences in programming. A PCA pump infuses pain medication and the patient presses a button to obtain pain medication at predetermined intervals.
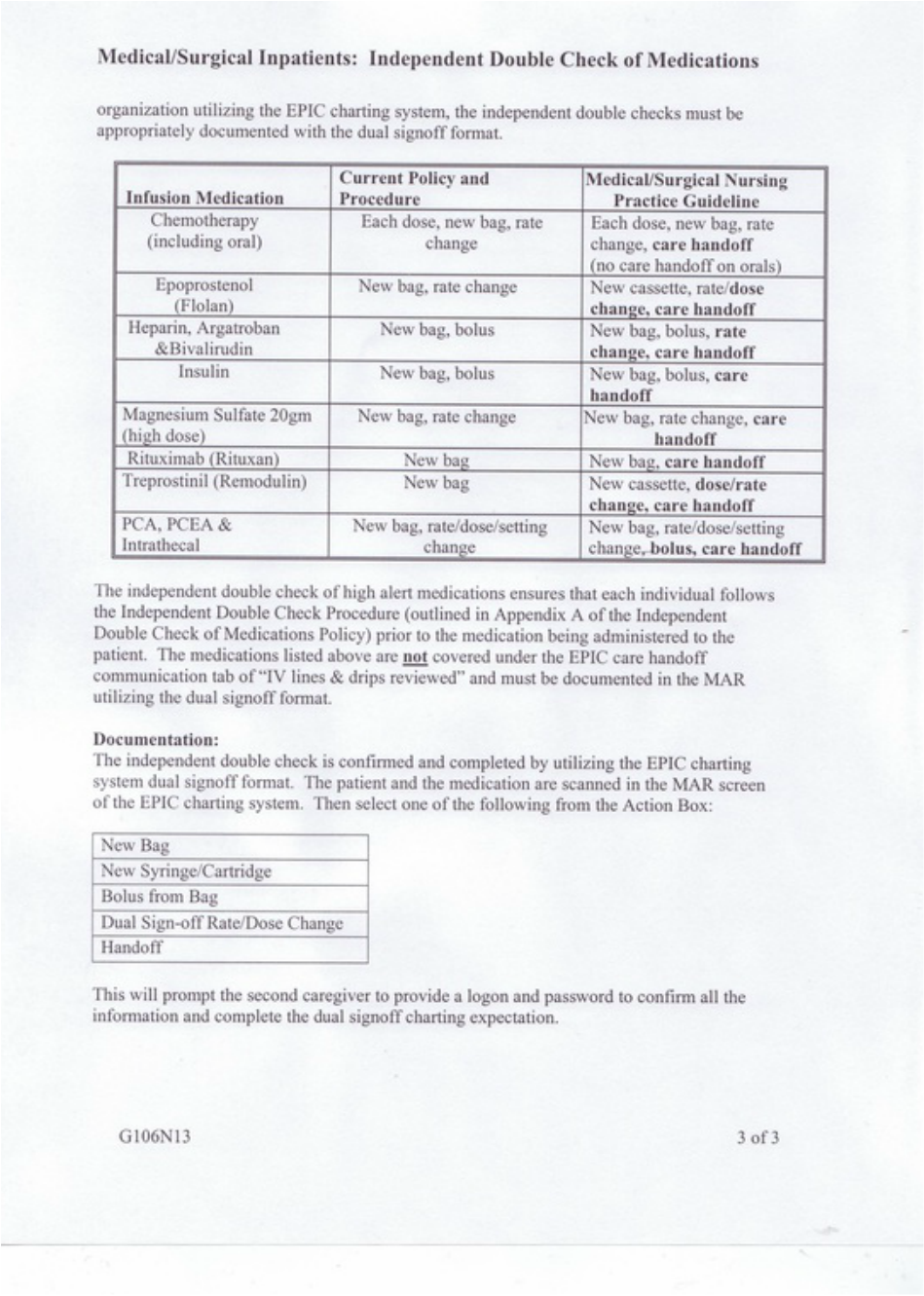
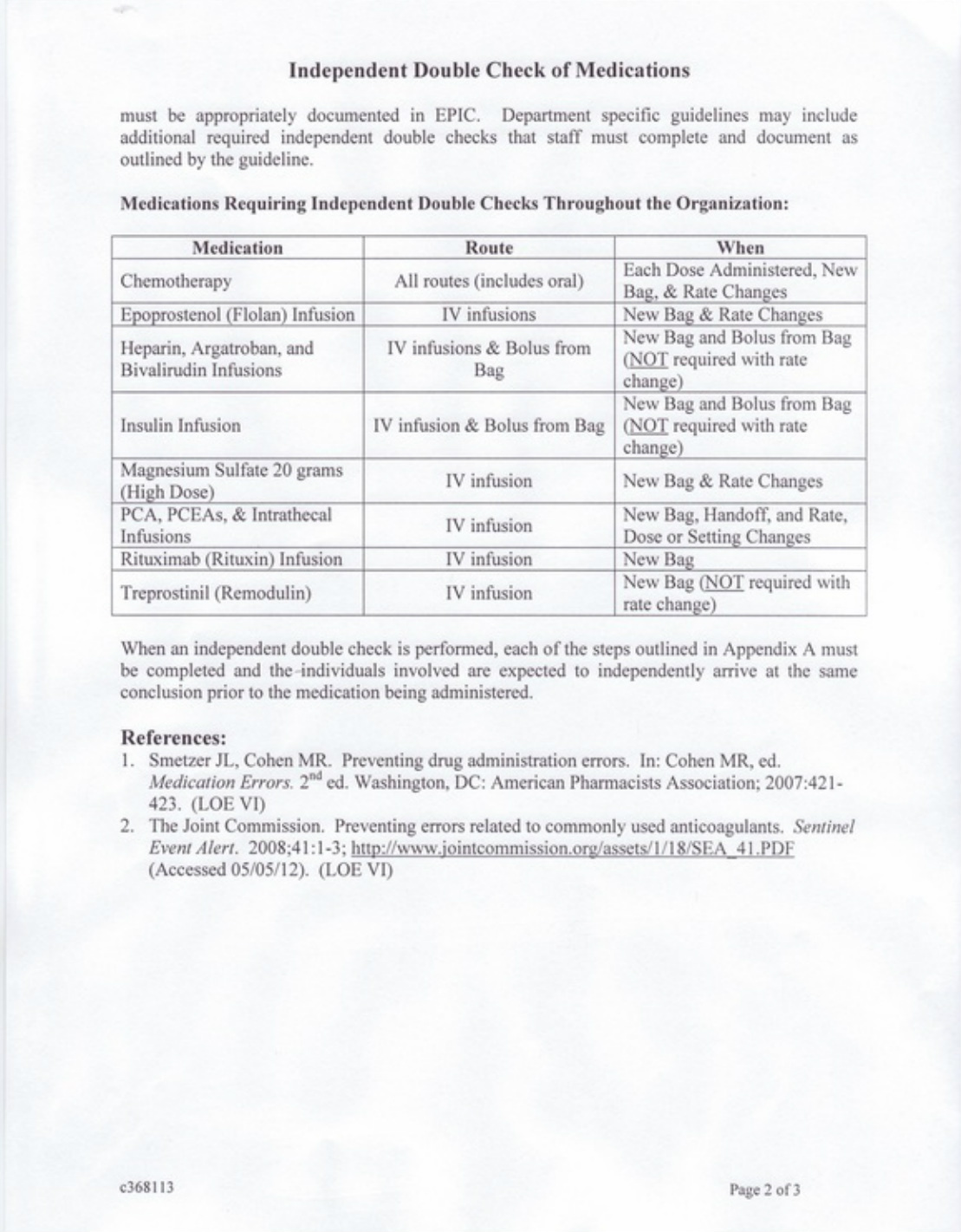
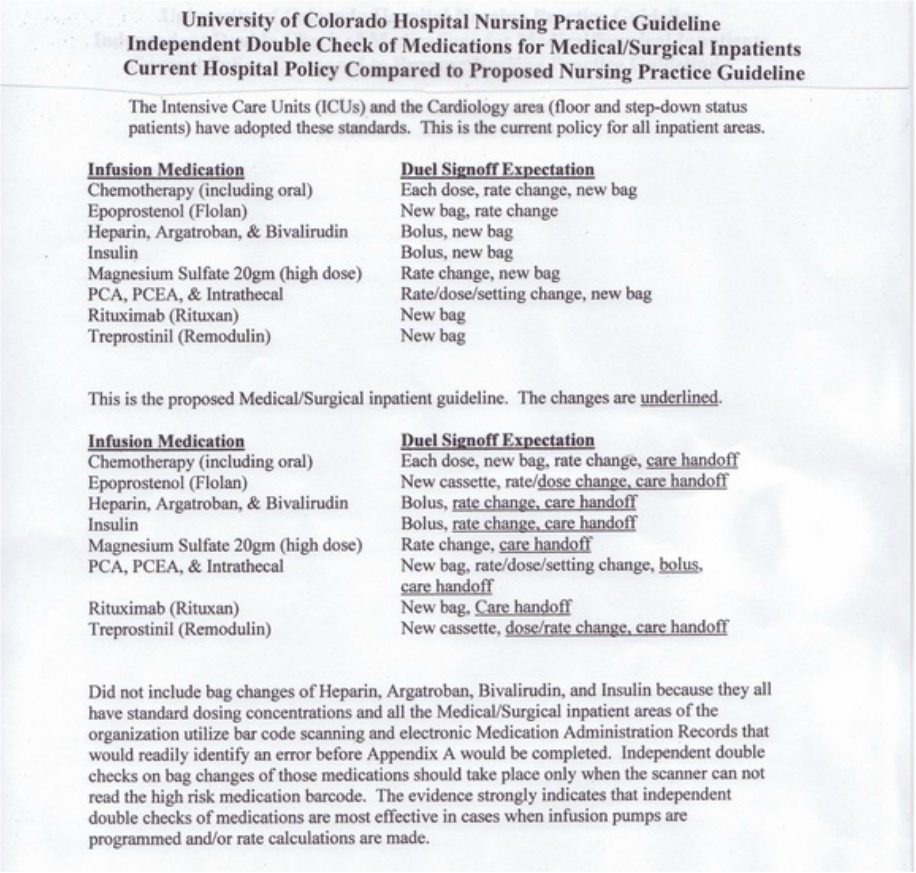
The updated policy did not address the issue of care handoff cosigning. This was an area of confusion and inconsistency throughout the hospital. When patient care is transferred from one RN to another RN, all high risk medication infusions are verified and cosigned in the EPIC charting system. This provides a smooth transition for the patient and validates dosages and rates of high risk infusions. Until this guideline was established, there was no consistency with what specific medications would require an independent double check and what specific component of the medication would require an independent double check. The nursing practice guideline contains a chart that displays the current Policy and Procedure that was adapted to the Medical/Surgical areas of the hospital. Note the significant policy changes that are in bold print.
The unit educator and I were reviewing the policy shown above, that directly affected the Pulmonary Unit. The Independent Double Check of High Risk Medications Policy did not require an independent double check of dose changes for Epoprostenol (Flolan) and Treprostinil (Remodulin). The administration and monitoring of these medications are one of the specialties of the Pulmonary Unit. It is routine practice to independently double check and cosign all dosage changes with two Registered Nurses (RN) of this medication that treats pulmonary hypertension with a continuous infusion through a pump that looks similar to the traditional Patient Controlled Analgesia (PCA) pump but has significant differences in programming. A PCA pump infuses pain medication and the patient presses a button to obtain pain medication at predetermined intervals.
The updated policy did not address the issue of care handoff cosigning. This was an area of confusion and inconsistency throughout the hospital. When patient care is transferred from one RN to another RN, all high risk medication infusions are verified and cosigned in the EPIC charting system. This provides a smooth transition for the patient and validates dosages and rates of high risk infusions. Until this guideline was established, there was no consistency with what specific medications would require an independent double check and what specific component of the medication would require an independent double check. The nursing practice guideline contains a chart that displays the current Policy and Procedure that was adapted to the Medical/Surgical areas of the hospital. Note the significant policy changes that are in bold print.
The entire process began with reviewing the Independent Double Check of Medications Policy, The PCA Policy, the Epidural (PCEA) Policy, and the practice guidelines of all the remaining medications. The primary concern was what specific components of the medication should have an independent double check performed.
The next step was to review the Patient Safety Net (PSN) submissions that directly related to these medications. I collaborated with Lindsie Klingman who is our Quality Improvement Specialist. There were over 200 PSN submissions on Heparin alone. I reviewed numerous PSN submissions with rate change errors for Heparin, Argatroban, Bivalrudin, and Insulin. The vast majority of these medication errors could of been prevented if an independent double check was performed before the rate was changed. Most of these medication errors had occurred while the current policy was in place.
Heparin, Argatroban, and Bivalrudin rate changes are dictated by what the lab value is for a test of blood coagulation factors. This value is compared to the actual order in the Medication Administration Record (MAR) to determine how the infusion rate is adjusted. There are several variables that are involved in this process that can easily contribute to medication errors. These errors could be minimized if an independent double check was performed and both individuals came to the same conclusion.
Insulin rate changes present with similar difficulties. The rate change is dictated by multiple factors: the previous rate of infusion, the current rate of infusion, and the current blood glucose level of the patient. These factors are compared to an insulin infusion chart to determine the value of the rate change. The PSN submissions displayed numerous errors with insulin rate changes. These errors could be significantly decreased if an
independent double check was performed and both individuals came to the same conclusion.
The next step was to review the literature. There were studies that displayed significant reduction in medication errors when an independent double check was performed. Several journal articles concluded that independent double check of medications should be performed on any instance where multiple steps are performed for rate and dosage changes. The literature review cited independent double check of medications as a primary strategy to reduce medication errors. The current policy did not address these critical factors.
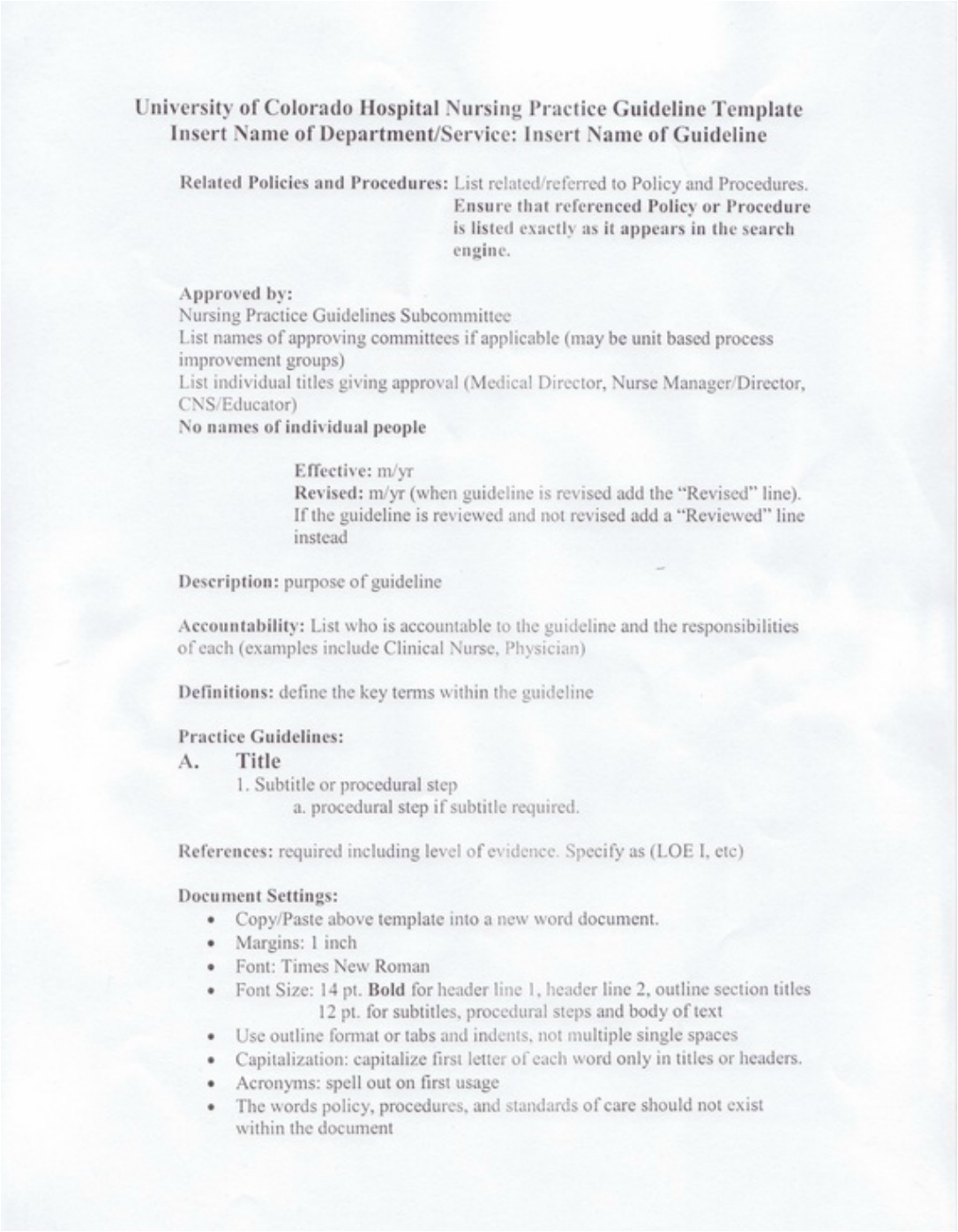
The next step was to put all this information into a concise, thorough, and easy to read guideline. The current trend was to have all policy, procedure, and guidelines available on the hospital's website called the HUB and stray away from unit based binders that are practically outdated shortly after they are assembled. Below is the template that was utilized.
The next step was to review the Patient Safety Net (PSN) submissions that directly related to these medications. I collaborated with Lindsie Klingman who is our Quality Improvement Specialist. There were over 200 PSN submissions on Heparin alone. I reviewed numerous PSN submissions with rate change errors for Heparin, Argatroban, Bivalrudin, and Insulin. The vast majority of these medication errors could of been prevented if an independent double check was performed before the rate was changed. Most of these medication errors had occurred while the current policy was in place.
Heparin, Argatroban, and Bivalrudin rate changes are dictated by what the lab value is for a test of blood coagulation factors. This value is compared to the actual order in the Medication Administration Record (MAR) to determine how the infusion rate is adjusted. There are several variables that are involved in this process that can easily contribute to medication errors. These errors could be minimized if an independent double check was performed and both individuals came to the same conclusion.
Insulin rate changes present with similar difficulties. The rate change is dictated by multiple factors: the previous rate of infusion, the current rate of infusion, and the current blood glucose level of the patient. These factors are compared to an insulin infusion chart to determine the value of the rate change. The PSN submissions displayed numerous errors with insulin rate changes. These errors could be significantly decreased if an
independent double check was performed and both individuals came to the same conclusion.
The next step was to review the literature. There were studies that displayed significant reduction in medication errors when an independent double check was performed. Several journal articles concluded that independent double check of medications should be performed on any instance where multiple steps are performed for rate and dosage changes. The literature review cited independent double check of medications as a primary strategy to reduce medication errors. The current policy did not address these critical factors.
The next step was to put all this information into a concise, thorough, and easy to read guideline. The current trend was to have all policy, procedure, and guidelines available on the hospital's website called the HUB and stray away from unit based binders that are practically outdated shortly after they are assembled. Below is the template that was utilized.
1. Drafts
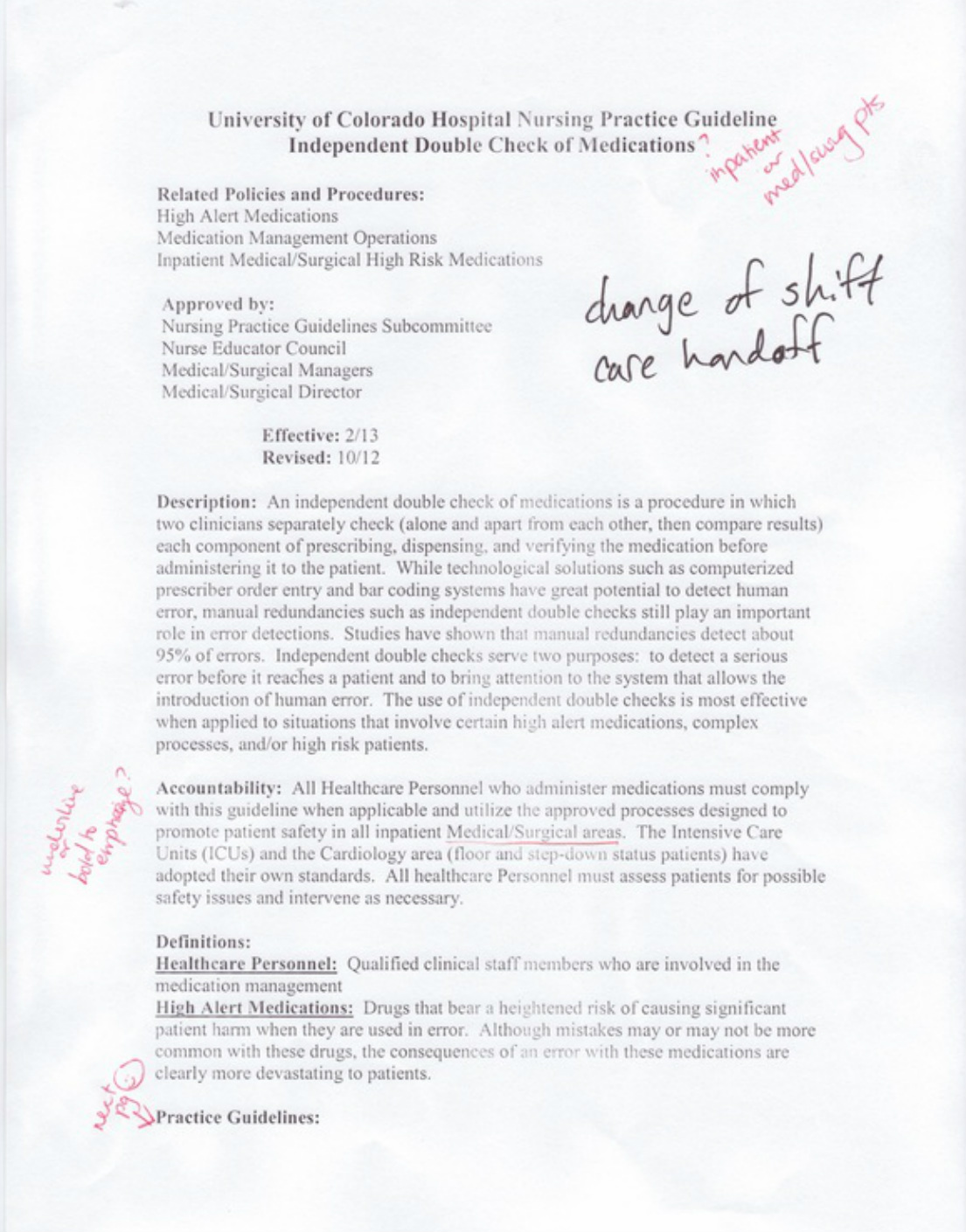
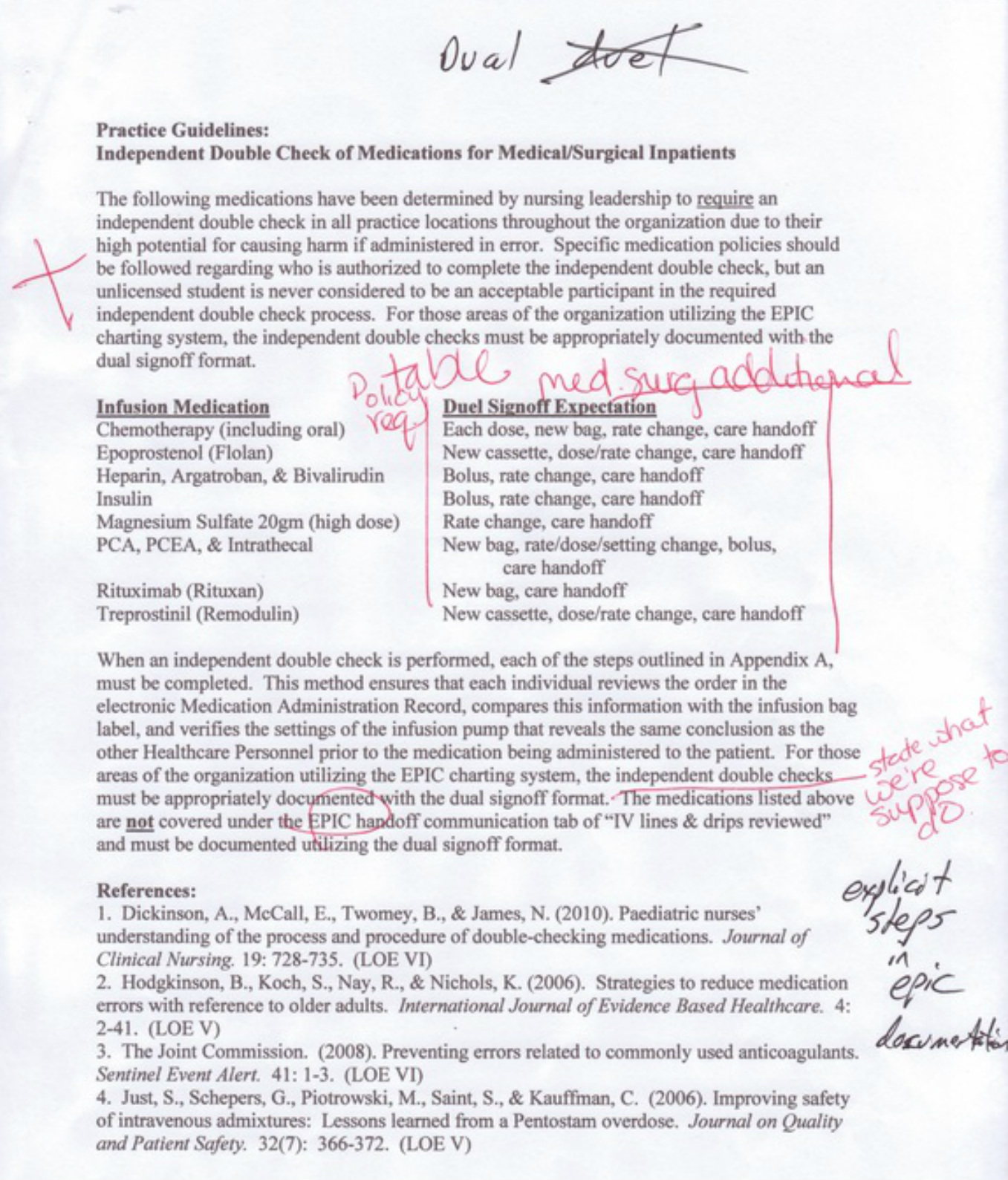
Draft #1 of the first page with corrections
Draft #1 of the first page with corrections
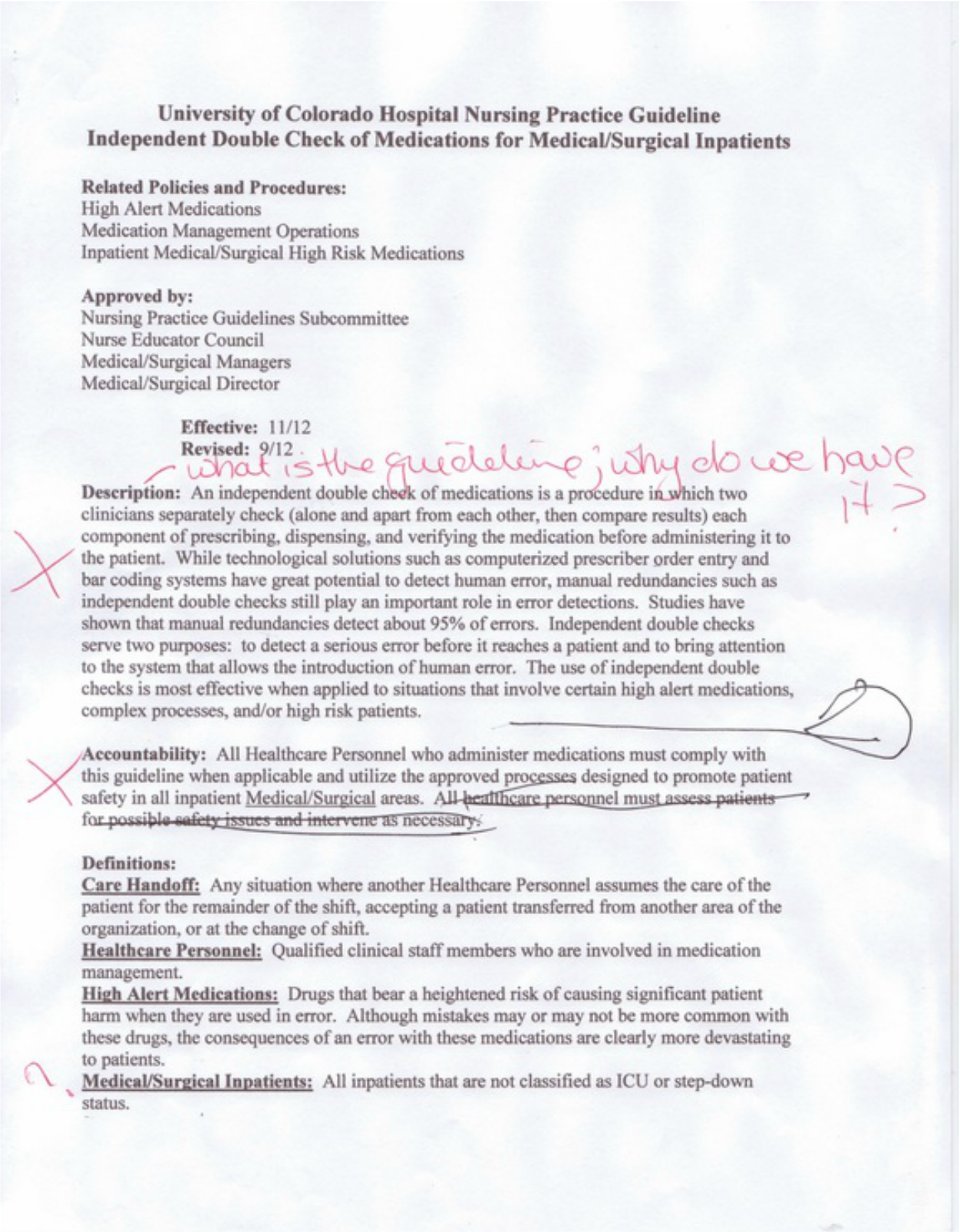
Draft #2 of the first page with corrections
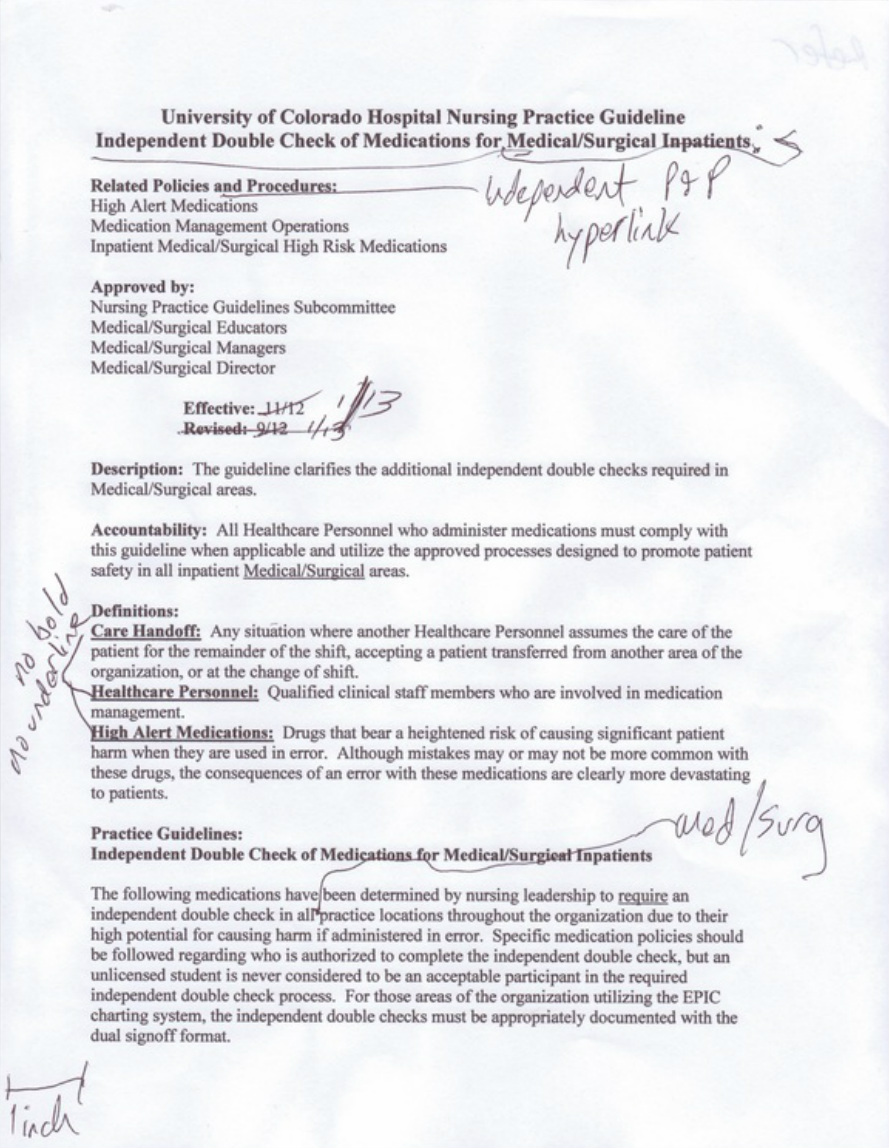
Draft #3 of the first page with corrections
Draft #1 of the second page
Draft #2 of the second page with corrections
Draft #3 of the guideline expectations with corrections
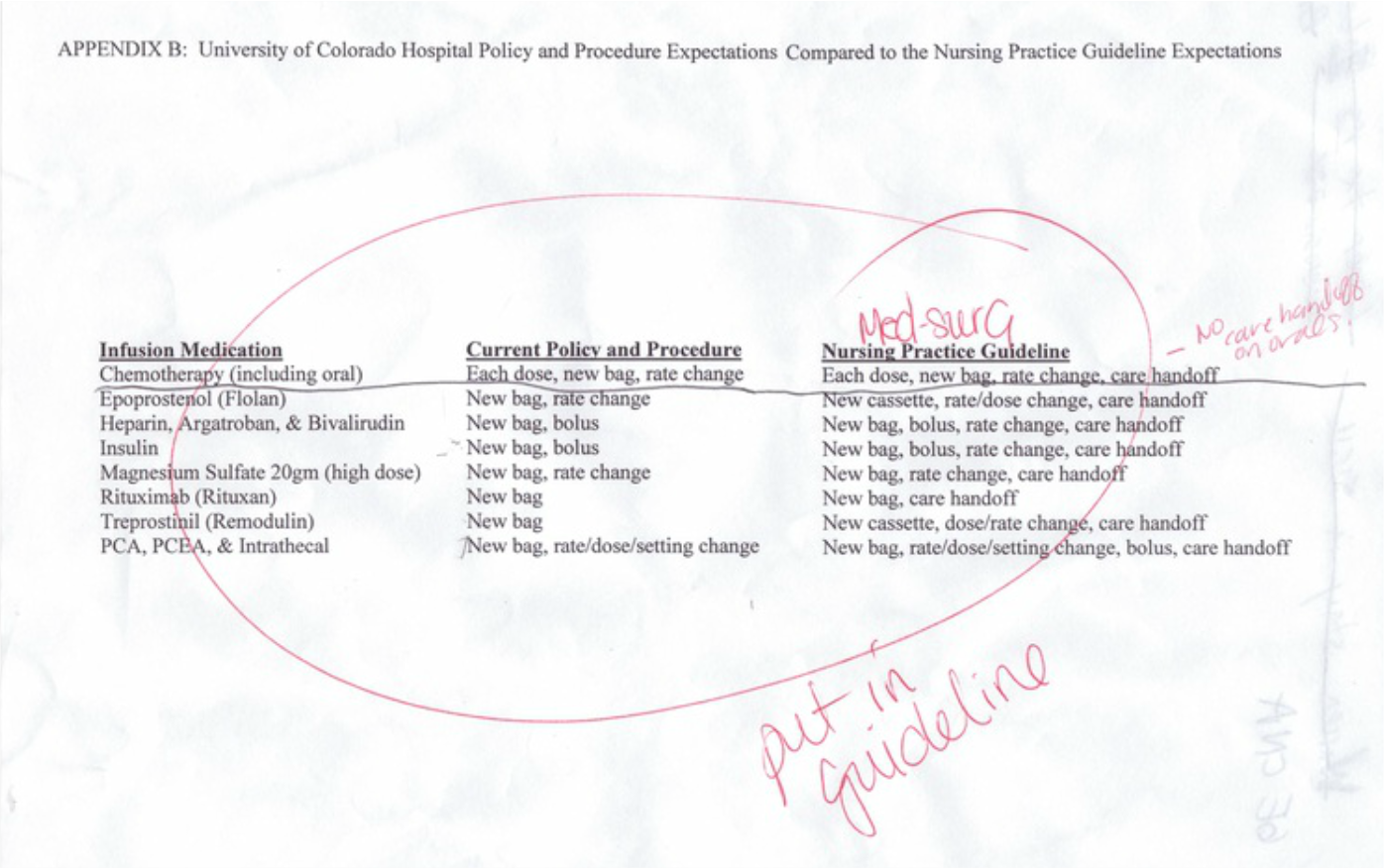
Draft #4 of the guideline expectations with corrections
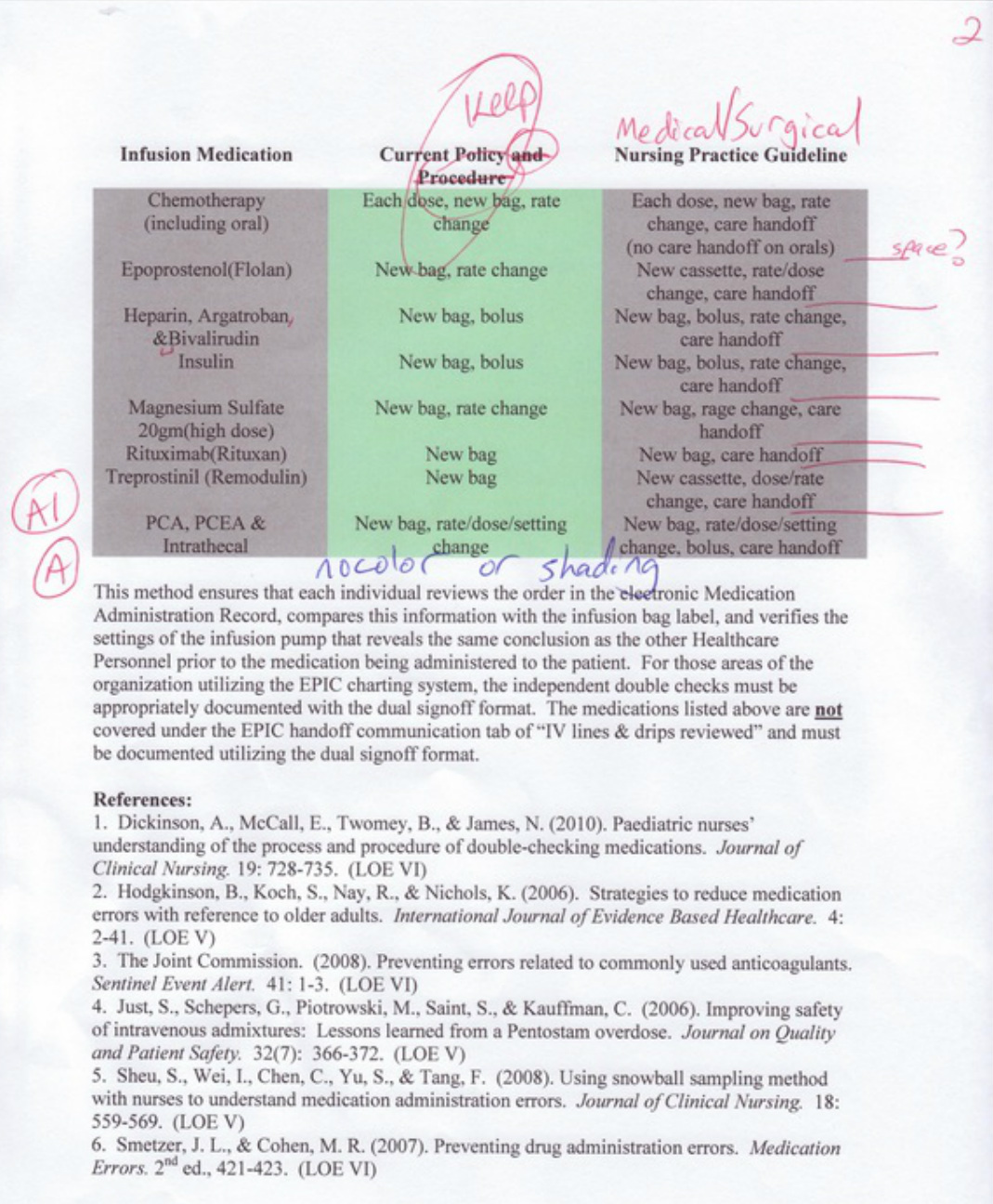
Draft #5 of the guideline expectations with corrections
The final draft was ready for the committee reviews. I must thank Katie Creviston, the Pulmonary Unit's educator for her thoughts and suggestions that assisted in transforming the drafts into the final production.